- Dislocated shoulder
-
Dislocated shoulder Classification and external resources 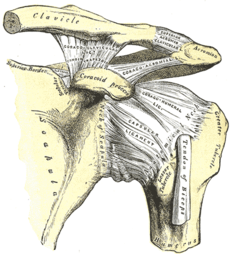
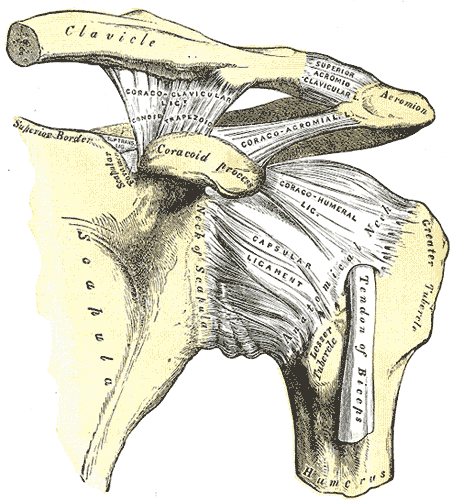
The left shoulder and acromioclavicular joints, and the proper ligaments of the scapula.ICD-10 S43.0 ICD-9 831 DiseasesDB 31231 eMedicine orthoped/440 radio/630 sports/152 MeSH D012783  A anterior dislocation of the shoulder
A anterior dislocation of the shoulder
 An inferior dislocation of the shoulder after a car accident. Note how the humerus is abducted. As present is a fracture of the greater tuberosity.
An inferior dislocation of the shoulder after a car accident. Note how the humerus is abducted. As present is a fracture of the greater tuberosity.A dislocated shoulder occurs when the humerus separates from the scapula at the glenohumeral joint. The shoulder joint has the greatest range of motion of any joint in the body and as a result is particularly susceptible to dislocation and subluxation.[1] Approximately half of major joint dislocations seen in emergency departments are of the shoulder. Partial dislocation of the shoulder is referred to as subluxation.
Contents
Classification
Anterior (forward)
Over 95% of shoulder dislocation cases are anterior. Most anterior dislocations are sub-coracoid. Sub-glenoid; subclavicular; and, very rarely, intrathoracic or retroperitoneal dislocations may occur.[2]
It can result in damage to the axillary artery.[3]
Posterior (backward)
Posterior dislocations are occasionally due to electric shock or seizure and may be caused by strength imbalance of the rotator cuff muscles. Posterior dislocations often go unnoticed, especially in an elderly patient[4] and in the unconscious trauma patient.[5] An average interval of 1 year was discovered between injury and diagnosis of posterior dislocation in a series of 40 patients.[6]
Inferior (downward)
Inferior dislocation is the least likely form, occurring in less than 1% of all shoulder dislocation cases. This condition is also called luxatio erecta because the arm appears to be permanently held upward or behind the head.[7] It is caused by a hyper abduction of the arm that forces the humeral head against the acromion. Inferior dislocations have a high complication rate as many vascular, neurological, tendon, and ligament injuries are likely to occur from this kind of dislocation.
Signs
- Significant pain, which can sometimes be felt past the shoulder, along the arm.
- Inability to move the arm from its current position, particularly in positions with the arm reaching away from the body and with the top of the arm twisted toward the back.
- Numbness of the arm.
- Visibly displaced shoulder. Some dislocations result in the shoulder appearing unusually square.
- No bone in the side of the shoulder showing shoulder has become dislocated.
Treatment
Initial
Prompt professional medical treatment should be sought for any suspected dislocation injury. Usually, a dislocated shoulder is kept in its current position by use of a splint or sling (however, see below). A pillow between the arm and torso may provide support and increase comfort. Strong analgesics are needed to allay the pain of a dislocation and the anxiety associated with it, and hence, conservative measures of pain relief should not be attempted.
Emergency department care is focused on returning the shoulder to its normal position via processes known as reduction. Normally, closed reduction, in which several methods are used to manipulate the bone and joint from the outside, is used. A variety of techniques exist, but some are preferred due to fewer complications or easier execution.[8] In cases where closed reduction is not successful, surgical open reduction may be needed.[9] Following reduction, X-Ray imaging is often used to ensure that the reduction was successful and there are no fractures. The arm should be kept in a sling or immobilizer for several days, preferably until orthopedic consultation. Hippocrates' and Kocher's method are rarely used anymore. Hippocrates used to place the heel in the axilla and reduce shoulder dislocations. Kocher's method, if performed patiently and slowly, can be performed without anesthesia and if done correctly does not cause pain. Traction is applied on the arm and it is abducted. Then, it is externally rotated, and the arm is adducted following which it is internally rotated and maintained in the position with the help of a sling. A chest x-ray should be taken to confirm whether the head of humerus has reduced back into the glenoid cavity. This methodology is performed with external rotation of shoulder, and adduction of the elbow. Some do not recommend it because of possible neurovascular complications and proximal humerus fractures.
If no medical help is available, fairly simple methods can be attempted, such as Milch's method, or Stimson's Method (anterior dislocations).
In Australia, an anterior dislocation reduction method that is commonly used is the Spaso technique[10]. This technique was first used by Spaso Miljesic a plaster technician at Western Health, Melbourne, Australia. The technique is reliable and simple. Holding the patient's wrist, gently flex the arm at the shoulder joint with an extended elbow until 90 degrees is achieved. Then apply gentle traction and external rotation. Listen for a clunk indicating relocation. If the patient experiences pain and muscle spasm, wait until it subsides and gently continue. Procedural sedation may be useful. A recent study[11] found the Spaso technique useful in 87.5% of cases of anterior dislocation with no complications.
Post-reduction: immobilisation in external versus internal rotation
For thousands of years, treatment of anterior shoulder dislocation has included immobilisation of the patient's arm in a sling, with the arm placed in internal rotation (across the body). However, three studies, one in cadavers and two in patients, suggest that the detachment of the structures in the front of the shoulder is made worse when the shoulder is placed in internal rotation to be seen. By contrast, the structures are realigned when the arm is placed in external rotation. New data suggest that if the shoulder is managed non-operatively and immobilised, it should be immobilised in a position of external rotation.[12][13]
Another study found that conventional shoulder immobilisation in a sling offered no benefit.[14]
Surgery
 MRI of shoulder after dislocation with Hill-Sachs lesion and labral Bankart's lesion.
MRI of shoulder after dislocation with Hill-Sachs lesion and labral Bankart's lesion.Some cases require non-emergency surgery to repair damage to the tissues surrounding in the shoulder joint and restore shoulder stability. Arthroscopic surgery techniques may be used to repair the glenoidal labrum, capsular ligaments, biceps long head anchor or SLAP lesion and/or to tighten the shoulder capsule.[15]
The time-proven surgical treatment for recurrent anterior instability of the shoulder is a Bankart repair.[16] Surgery to anatomically and securely repair the torn anterior glenoid labrum and capsule without arthroscopy can lessen pain and improve function for active individuals. When the front of the shoulder socket has been broken or worn, a bone graft may be required to restore stability.[17] When the shoulder dislocates posteriorly (out the back), a surgery to reshape the socket may be necessary. Surgery to build up the back of the glenoid socket using an osteotomy and graft can restore shoulder anatomy and lessen pain and improve function. Conversely, there are new procedures that should be investigated as a possible alternative to open surgery.[18]
Non-operative
Rotator cuff and deltoid strengthening has long been the focus of conservative treatment for the unstable shoulder and in many cases is advocated as a substitute for surgical stabilization. In multidirectional instability patients who have experienced atraumatic subluxation or dislocation events, cohort studies demonstrate good responses to long-term progressive resistance exercises if judged according to function, pain, stability, and motion scores.[19] However, in those experiencing a discrete traumatic dislocation event, responses to non-operative treatment are less than satisfactory, a pattern that inspired the Matsen and Harryman classification of shoulder instability, TUBS (traumatic, unidirectional, Bankart, and usually requiring surgery) and AMBRI (atraumatic, multidirectional, bilateral, rehabilitation, and occasionally requiring an inferior capsular shift).[20] It is thought that traumatic dislocations, as opposed to atraumatic dislocations and instability events, result in a higher incidence of capsuloligamentous injuries that disturb normal anatomy and leave shoulders too structurally compromised to respond to conservative treatment. Pathoanatomic studies of first-time traumatic anterior dislocators reveal a high rate of labral lesions including Bankart lesions.[21]
See also
References
- ^ Thomas C. Schuler,M.D., F.A.C.S Curr Opin Pediatr. 2005 Feb;17(1):25-9.http://www.spinemd.com/publications/articles/traumatic-shoulder-dislocation-in-the-adolescent-athlete-advances-in-surgical-treatment
- ^ Shoulder Dislocations at eMedicine
- ^ Kelley SP, Hinsche AF, Hossain JF (November 2004). "Axillary artery transection following anterior shoulder dislocation: classical presentation and current concepts". Injury 35 (11): 1128–32. doi:10.1016/j.injury.2003.08.009. PMID 15488503. http://linkinghub.elsevier.com/retrieve/pii/S0020138303003346.
- ^ Dislocations, Shoulder at eMedicine
- ^ Life in the Fast Lane Posterior Shoulder Dislocation
- ^ Hawkins RJ, Neer CS, Pianta RM, Mendoza FX (January 1987). "Locked posterior dislocation of the shoulder". J Bone Joint Surg Am 69 (1): 9–18. PMID 3805075. http://www.medscape.com/medline/abstract/3805075?src=emed_ckb_ref_0.
- ^ Dislocations, Shoulder~clinical at eMedicine
- ^ Dislocations, Shoulder~workup at eMedicine
- ^ Dislocated shoulder: Treatment - MayoClinic.com
- ^ Miljesic, Kelly; Kelly, Anne-Maree (1998). "Reduction of anterior dislocation of the shoulder: the Spaso technique". Emergency Medicine Australasia 10 (2): 173–175. doi:10.1111/j.1442-2026.1998.tb00676.x. http://onlinelibrary.wiley.com/doi/10.1111/j.1442-2026.1998.tb00676.x/abstract.
- ^ Yuen, Gap, Chan, Tung (2001). "An easy method to reduce anterior shoulder dislocation: the Spaso technique". Emerg Med J 18 (5): 370–372. doi:10.1136/emj.18.5.370. PMC 1725682. PMID 11559608. http://emj.bmj.com/content/18/5/370.abstract.
- ^ Murrell GA (October 2003). "Treatment of shoulder dislocation: is a sling appropriate?". Med. J. Aust. 179 (7): 370–1. PMID 14503903. http://www.mja.com.au/public/issues/179_07_061003/mur10335_fm.html.
- ^ http://www.ori.org.au/bonejoint/shoulder/ssfd.htm
- ^ Chalidis B, Sachinis N, Dimitriou C, Papadopoulos P, Samoladas E, Pournaras J (June 2007). "Has the management of shoulder dislocation changed over time?". Int Orthop 31 (3): 385–9. doi:10.1007/s00264-006-0183-y. PMC 2267594. PMID 16909255. http://www.springerlink.com/content/e845216618wj6247/.
- ^ Considering surgery - Arthroscopic shoulder surgery for dislocation, subluxation, and instability: why, when and how it is done
- ^ "Bankart repair for unstable dislocating shoulders:". University of Washington: Orthopaedics and Sports Medicine. http://www.orthop.washington.edu/openbankart.
- ^ "Anterior glenoid reconstruction for unstable dislocating shoulders.". University of Washington: Orthopaedics and Sports Medicine. http://www.orthop.washington.edu/shoulderbonegraft.
- ^ "Thermal Capsulorrhaphy". American Academy of Orthopaedic Surgeons. http://orthoinfo.aaos.org/topic.cfm?topic=A00034.
- ^ Treatment of instability of the shoulder with an exercise program. Burkhead,W.Z.,Jr; Rockwood,C.A.,Jr. J.Bone Joint Surg.Am., 1992, 74, 6, 890-896.
- ^ Matsen FA III, Harryman DT II, Sidles JA. Mechanics of glenohumeral instability. Clin Sports Med 1991;10:783-788.
- ^ Owens, B. D., Nelson, B. J., Duffey, M. L., Mountcastle, S. B., Taylor, D. C., Cameron, K. L., et al. (2010). Pathoanatomy of first-time, traumatic, anterior glenohumeral subluxation events. The Journal of Bone and Joint Surgery.American Volume, 92(7), 1605-1611.
External Links
Injury: Dislocations/subluxations, sprains and strains (Sx3 where x=0 to 9, 830–848) Joints and
ligamentsHead and neckShoulder and upper armMuscles and
tendonsShoulder and upper armM: JNT
anat(h/c, u, t, l)/phys
noco(arth/defr/back/soft)/cong, sysi/epon, injr
proc, drug(M01C, M4)
Categories:- Injuries of shoulder and upper arm
- Shoulder
- Dislocations, sprains and strains



Wikimedia Foundation. 2010.