- Sudden infant death syndrome
-
Sudden infant death syndrome Classification and external resources ICD-10 R95 ICD-9 798.0 OMIM 272120 DiseasesDB 12633 eMedicine emerg/406 ped/2171 MeSH D013398 Sudden infant death syndrome (SIDS) is marked by the sudden death of an infant that is unexpected by medical history, and remains unexplained after a thorough forensic autopsy and a detailed death scene investigation. An infant is at the highest risk for SIDS during sleep, which is why it is sometimes referred to by the terms cot death or crib death. The cause of SIDS is unknown, but characteristics associated with the syndrome have been identified. One of these characteristics is sleeping in the prone position. There are many risk factors and medical causal relationships associated with SIDS. Infants exposed to tobacco smoke are at risk. Infanticide and child abuse cases are misdiagnosed as SIDS due to lack of evidence.[1][2] Accidental suffocations are sometimes misdiagnosed as SIDS.[citation needed] Genetics play a role, as SIDS is more prevalent in males.[3][4] Safe sleep environments that reduce the risk of SIDS include proper ventilation, and putting infants on their back to sleep.[5] Pacifiers and tummy time can help reduce known risk factors.[6]
Contents
Definition
Typically the infant is found dead after having been put to bed, and exhibits no signs of having suffered.[7]
SIDS is a diagnosis of exclusion. It should only be applied to an infant whose death is sudden and unexpected and remains unexplained after the performance of an adequate postmortem investigation including:
- an autopsy (by an experienced pediatric pathologist, if possible);
- investigation of the death scene and circumstances of the death;
- exploration of the medical history of the infant and family.
Australia and New Zealand are shifting to the term "sudden unexplained death in infancy" (SUDI) for professional, scientific and coronial clarity.
The term SUDI is now often used instead of sudden infant death syndrome (SIDS) because some coroners prefer to use the term 'undetermined' for a death previously considered to be SIDS. This change is causing diagnostic shift in the mortality data.[8]
In addition, the U.S. Centers for Disease Control and Prevention (CDC) has recently suggested that such deaths be called "sudden unexpected infant deaths" (SUID) and that SIDS is a subset of SUID.[9]
Risk factors
The cause of SIDS is unknown. Although studies have identified risk factors for SIDS, such as putting infants to bed on their stomachs, there has been little understanding of the syndrome's biological cause or potential causes. The frequency of SIDS appears to be a strong function of the infant's sex, age and ethnicity, and the education and socio-economic-status of the infant's parents.
Listed below are several risk factors associated with increased probability of the syndrome.
Before birth
- teenage mother (SIDS rates decrease with increasing maternal age)[10]
- lack of prenatal care (SIDS rates increase with increasing delay in starting pre-natal care)[10]
- exposure to nicotine by maternal smoking (SIDS rates are higher for infants of mothers who smoke during pregnancy)[10][11]
After birth
- mold (can cause bleeding lungs plus a variety of other uncommon conditions leading to a misdiagnosis and death). It is often misdiagnosed as a virus, flu, and/or asthma-like conditions.[12]
- low birth weight (in the US from 1995-1998 the rate for 1000-1499 g was 2.89/1000 and for 3500-3999 g it was 0.51/1000)[13][14]
- exposure to tobacco smoke[15]
- prone sleep position (lying on the stomach, see sleep positioning below)[16][17]
- not breastfeeding[18]
- elevated or reduced room temperature[19]
- excess bedding, clothing, soft sleep surfaces and stuffed animals[20]
- co-sleeping with parents or other siblings may increase risk for SIDS, but the mechanism remains unclear[21]
- infant's age (incidence rises from zero at birth, is highest from two to four months, and declines towards zero at one year)[22]
- premature birth (increases risk of SIDS death by about four times.[10][13] In 1995-1998 the US SIDS rate for 37–39 weeks of gestation was 0.73/1000; The SIDS rate for 28–31 weeks of gestation was 2.39/1000)[13]
- anemia[23] [NB: per item 6 in the list of epidemiologic characteristics below, extent of anemia cannot be evaluated at autopsy because "total hemoglobin can only be measured in living infants.[24]"
Hypotheses
Bacterial Infections
In a British study released May 29, 2008 researchers discovered that the common bacterial infections Staphylococcus aureus (staph) and Escherichia coli (E. coli) appear to be a risk factor in some cases of SIDS. Both bacteria were present at greater-than-usual concentrations in infants who died from SIDS.[25] SIDS cases peak between eight and ten weeks after birth, which is also the time frame in which the antibodies that were passed along from mother to child are starting to disappear and babies have not yet made their own antibodies.
Bed Sharing
A 2005 policy statement by the American Academy of Pediatrics on sleep environment and the risk of SIDS deemed co-sleeping and bed sharing unsafe.[26] One article reports that co-sleeping infants have a greater risk of airway covering than when the same infant sleeps alone in a cot, but came to the conclusion that "Although numerous authors have suggested that bed-sharing infants face risks because of airway covering by bed-clothes or parental bodies, the present trial does not lend support to this hypothesis".[27]
Brain disorders
According to a JAMA 2006 study some babies who die of SIDS have abnormalities in the brain stem (the medulla oblongata) of underdevelopment of receptors for serotonin, which help control functions like breathing, blood pressure and arousal, and abnormalities in serotonin signaling. According to the National Institutes of Health, this finding was the strongest evidence at that time that structural differences in a specific part of the brain may contribute to the risk of SIDS.[28] This abnormality can continue postpartum until the end of the first year. This could account for there being few SIDS deaths after the first year of infancy and the reason the risk is greater for premature infants. The authors noted that males have fewer serotonin receptors than females, perhaps contributing to the increased incidence of SIDS in males, but their follow-up 2010 paper failed to reconfirm that gender difference.[29]
Another 2006 study showed that a possible cause of SIDS is because parents leave their infants in a position known as the Trendelenburg position.[30] This position can cause the brain stem to fall, and in a result, the brain becomes "crushed". The proper position for an infant is either Fowler's position or Sims'.[citation needed]
A 2010 study suggests Interleukin-2, a neuromodulator, as the potential mechanism. Intense neuronal IL-2 immune-reactivity in the SIDS brainstem was found, which could be responsible for decreased cardiorespiratory and arousal responses.[31]
Central respiratory pattern deficiency
There is ongoing research in the pediatric/neonatal community that has begun to associate apnea-like breathing cessations in animal models with unusual neural architecture or signal transduction in central pattern generator circuits including the pre-Bötzinger complex.[32]
Cervical spinal injury from birth trauma
During birth, if the infant's head is traumatically turned side to side, upper cervical spinal injury can result. Difficulty breathing is a classic sign of upper spinal cord and brain-stem injury.[33] When infants with undiagnosed upper cervical spinal cord injury are continually placed on their stomach for sleep, they are forced to turn their head to the side to breathe.
Child abuse
Several instances of infanticide have been uncovered where the diagnosis was originally SIDS.[1][2] This has led some researchers to estimate that 5% to 20% of SIDS deaths are infanticides.[34][35][36][37] In 1997 The New York Times, covering a book called The Death of Innocents: A True Story of Murder, Medicine and High-Stakes Science, wrote:
The misdiagnosis of infanticide as SIDS "happens all over," Ms. Talan, a medical reporter at Newsday, said. "A lot of doctors and police don't know how to handle it. They don't take it as seriously as they should." As a result of the book's revelations, people are starting to scrutinize possible cases of this "perfect crime," which involves no physical evidence and no witnesses.[38]
A pediatrician, Roy Meadow, from the UK believes that many cases diagnosed as SIDS are really the result of child abuse on the part of a parent. During the 1990s and early 2000s, a number of mothers of multiple apparent SIDS victims were convicted of homicide to various extents, on the basis of Meadow's opinion. In 2003 a number of high-profile acquittals brought Meadow's theories into disrepute. Several hundred murder convictions were reviewed, leading to several high-profile cases being re-opened and convictions overturned. Meadow was struck off in 2005.[39] Meadow appealed to the High Court, which ruled in his favour in February 2006. The GMC appealed to the Court of Appeal and in October 2006 by a majority decision, with the Master of the Rolls, Sir Anthony Clarke, dissenting, the Court of Appeal upheld the decision of the High Court in part ruling that Meadow's misconduct was not sufficiently serious to merit the punishment which he had received.
The Royal Statistical Society issued a media release refuting the expert testimony in one UK case in which the conviction was subsequently overturned.[40]
Genetics
There is a consistent 50% male excess in SIDS per 1000 live births of each sex. Given a 5% male excess birth rate (105 male to 100 female live births) there appear to be 3.15 male SIDS per 2 female SIDS for a male fraction of 0.61.[3][4] This value of 61% in the US is an average of 57% black male SIDS, 62.2% white male SIDS and 59.4% for all other races combined. Note that when multiracial parentage is involved, infant "race" is arbitrarily assigned to one category or the other; most often it is chosen by the mother. The X-linkage hypothesis for SIDS and the male excess in infant mortality have shown that the 50% male excess could be related to a dominant X-linked allele that occurs with a frequency of 1⁄3 that is protective of transient cerebral anoxia. An unprotected XY male would occur with a frequency of 2⁄3 and an unprotected XX female would occur with a frequency of 4⁄9. The ratio of 2⁄3 to 4⁄9 is 1.5 to 1 which matches the observed male 50% excess rate of SIDS.
Although many authors have found autosomal and mitochondrial genetic risk factors for SIDS they cannot explain the male excess because such gene loci have the same frequencies for males and females. Supporting evidence for an X-linkage is found by examination of other causes of infant respiratory death, such as suffocation by inhalation of food and other foreign objects. Although food is prepared identically for male and female infants, there is a similar 50% male excess of death from such causes indicating that males are more susceptible to the cerebral anoxia created by such incidents in exactly the same proportion as found in SIDS.[41][original research?]
The JAMA 2006 study which indicated that there was a relationship between fewer serotonin binding sites and SIDS noted that the boys "had significantly fewer serotonin binding sites than girls",[28] but the authors could not reproduce it in their 2010 paper.[29] However, such neurological prematurity decreases with age, but the male fraction of approximately 0.61 persists each month throughout the first year of life.[42] Furthermore, this cannot explain the identical male fraction of 0.61 in other respiratory mortality causes such as respiratory distress syndrome or suffocation from inhalation of food or foreign objects cited above, that also exists for all ages 1 to 14 years in the US from 1979 to 2005.[13][original research?]
Inner ear damage
Records of hearing tests (oto-acoustic emissions, OAEs) administered to certain infants show that those who later died of SIDS had differences in the pattern of these tests compared with normal babies. To be specific the OAE signal-to-noise ratio was reduced in the right ear in the SIDS babies (Rubens DD et al. Early Human Development 84, 225-9 (2008)).[43] It should be noted this was a small study (n=31 cases and 31 controls), had serious limitations (several significant factors were not controlled), and has been criticised from various perspectives.[44] The authors' suggestion for the cause of SIDS is that the deaths are caused by disturbances in respiratory control (other than suffocation). The vestibular apparatus of the inner ear has been shown to play an important role in respiratory control during sleep. It is speculated that this inner ear damage could be linked to SIDS. It is speculated that the damage occurs during delivery, particularly when prolonged contractions create greater blood pressure in the placenta. The right ear is directly in the "line of fire" for blood entering the fetus from the placenta, and thus could be most susceptible to damage. If the findings are relevant, it may be possible to take corrective measures. Researchers are beginning animal studies to explore the connection.[45]
Nitrogen dioxide
A 2005 study by researchers at the University of California, San Diego found that "SIDS may be related to high levels of acute outdoor NO2 exposure during the last day of life."[46] While nitrogen dioxide (NO2) exposure may be one of many possible risk factors, it is not considered causal, and the report cautioned that further studies were needed to replicate the result.
Toxic gases
In 1989, a controversial piece of research by UK Scientist Barry Richardson claimed that all cot deaths were the result of toxic nerve gases being produced through the action of fungus in mattresses on compounds of phosphorus, arsenic and antimony. These chemicals are frequently used to make mattresses fire-retardant.[citation needed]
Support for this hypothesis was based on the observation that the risk of cot death rises from one sibling to the next.[citation needed] Richardson claimed that parents are more likely to buy new bedding for their first child, and to re-use that bedding for later children. The more frequently used the bedding is, the more chance there will be that fungus has become resident in the material; thus, a higher chance of cot death. A paper by Peter Fleming and Peter Blair[47] references evidence from other studies that both supports and refutes the increasing occurrence of SIDS with mattress sharing and suggests that this is still inconclusive.
Dr. Jim Sprott recommends new parents either buy bedding free of the toxic compounds or to wrap the mattresses in a barrier film to prevent the escape of the gases. Sprott claims that no case of cot death has ever been traced back to a properly manufactured or wrapped mattress.[48]
However, a final report of "The Expert Group to Investigate Cot Death Theories: Toxic Gas Hypothesis", published in May 1998, concluded that "there was no evidence to substantiate the toxic gas hypothesis that antimony- and phosphorus-containing compounds used as fire retardants in PVC and other cot mattress materials are a cause of SIDS. Neither was there any evidence to believe that these chemicals could pose any other health risk to infants."[49] The report also states that "in normal cot-like conditions it is not possible to generate toxic gas from antimony in mattresses" and "babies have also been found to die on wrapped mattresses."
According to Dr. Sprott, as of 2006, the New Zealand government has not reported any SIDS deaths when babies have slept on mattresses wrapped according to his method. While the Limerick report claims that babies have been found to die on wrapped mattresses, Dr. Sprott argues that a chemical analysis of the bedding should be performed. He additionally claims that this part of the report was flawed:
In February 2000 Dr Peter Fleming (a co-author of the Limerick Report and principal author of the UK CESDI Report) conceded that the claim that three babies in the United Kingdom had died of cot death on polythene-covered mattresses could not be substantiated.[50]
Vaccination
Vaccination does not increase the risk of SIDS, and may reduce the risk slightly.[51][52]
According to the US Centers for Disease Control and Prevention:
From 2 to 4 months old, babies begin their primary course of routine vaccinations. This is also the peak age for sudden infant death syndrome (SIDS). The timing of these two events has led some people to believe they might be related. However, studies have concluded that vaccines are not a risk factor for SIDS.[52]
Vitamin C
In the 1970s, high doses of vitamin C were touted as a preventive measure for SIDS,[53] although the claim was controversial even then.[54][55] Subsequent studies failed to support a preventive role for vitamin C in SIDS.[56] To the contrary, a 2009 study found that high levels of vitamin C were strongly associated with SIDS, possibly through a pro-oxidant interaction with iron.[57]
Differential diagnosis
Some conditions that may be undiagnosed and thus could be alternative diagnoses to SIDS include:
- medium-chain acyl-coenzyme A dehydrogenase deficiency (MCAD deficiency)[58]
- infant botulism[59]
- long QT syndrome (accounting for less than 2% of cases)[60]
- infections with the bacterium Helicobacter pylori[61]
- shaken baby syndrome and other forms of child abuse[62][63]
- overlying[64]
For example an infant with MCAD deficiency could have died by "classical SIDS" if found swaddled and prone with head covered in an overheated room where parents were smoking. Genes of susceptibility to MCAD and Long QT syndrome do not protect an infant from dying of classical SIDS. Therefore presence of a susceptibility gene, such as for MCAD, means the infant may have died either from SIDS or from MCAD deficiency. It is impossible for the pathologist to distinguish between them.
A 2010 study looked at 554 autopsies of infants in North Carolina that listed SIDS as the cause of death and suggested that many of these deaths may have been due to accidental suffocation. The study found that 69% of autopsies listed other possible risk factors that could lead to death such us unsafe bedding or sleeping with adults.[65]
Prevention
Air circulation with fan use
According to a study of nearly 500 babies published in the October 2008 Archives of Pediatrics & Adolescent Medicine, using a fan to circulate air correlates with a lower risk of sudden infant death syndrome. This is plausible because a prone sleeping baby with nose to the sleeping surface could rebreathe some of its exhaled breath which is enriched in CO2 and depleted in oxygen. A fan could increase the mixing of the exhalation into the room air and lessen the risk of SIDS related to infant hypoxia. Researchers took into account other risk factors and found that fan use was associated with a 72% lower risk of SIDS. Only 3% of the babies who died had a fan on in the room during their last sleep, the mothers reported. That compared to 12% of the babies who lived. Using a fan reduced risk most for babies in poor sleeping environments.[5] Author De-Kun li said that "the baby's sleeping environment really matters" and that "this seems to suggest that by improving room ventilation we can further reduce risk."[66]
However, Dr. John Olssen at East Carolina University has pointed out that this study had a number of methodological flaws, such as selection and recall bias, low enrollment numbers, and dissimilar study groups. Olssen argues that although fan use is probably not harmful, it should not be recommended as a means to reduce the risk of SIDS.[67]
Bedding
Product safety experts advise against using pillows, sleep positioners, bumper pads, stuffed animals, or fluffy bedding in the crib and recommend instead dressing the child warmly and keeping the crib "naked."[68][69]
Blankets should not be placed over an infant's head.[70] It has been recommended that infants should be covered only up to their chest with their arms exposed. This reduces the chance of the infant shifting the blanket over his or her head.
Breastfeeding
A 2003 study published in Pediatrics, which investigated racial disparities in infant mortality in Chicago, found that previously or currently breastfeeding infants in the study had 1/5 the rate of SIDS compared with non-breastfed infants, but that "it became nonsignificant in the multivariate model that included the other environmental factors". These results are consistent with most published reports and suggest that other factors associated with breastfeeding, rather than breastfeeding itself, are protective."[71] A single more recent study claims to show a significantly reduced incidence of SIDS in breastfed infants.[72]
Bumper pads
Bumper pads may be a contributing factor in SIDS deaths and should be removed. Health Canada, the Canadian government's health department, issued an advisory[73] recommending against the use of bumper pads, stating:
The presence of bumper pads in a crib may also be a contributing factor for Sudden Infant Death Syndrome (SIDS). These products may reduce the flow of oxygen rich air to the infant in the crib. Furthermore, proposed theories indicate that the rebreathing of carbon dioxide plays a role in the occurrence of SIDS.
Concerns regarding recommendations
Dr. Rafael Pelayo from Stanford University and a number of other pediatric sleep researchers in the US have stated that they believe that the American Academy of Pediatrics' recommendations regarding cosleeping and pacifier use may have unintended consequences. They have stated that the SIDS prevention strategy of the American Academy of Pediatrics which keeps infants at a low arousal threshold and reduces the time in quiet sleep may be unhealthy for children. They state that slow wave sleep is the most restorative form of sleep and limiting this sleep in the first 12 months of life may have unintended consequences to both the sleep and the infant.[74]
According to a 1998 study by British researchers that compared back sleeping infants to stomach sleeping infants there were developmental differences at 6 months of age between the two groups. At 6 months of age the stomach sleeping infants had higher gross motor scores, social skills scores, and total development skills scores than the back sleeping infants. The differences were apparent at the 5% statistical significant level. But, at 18 months the differences were no longer apparent. The researchers deemed the lower development scores of back sleeping infants at 6 months of age to be transient and stated that they do not believe the back sleeping recommendations should be changed.[75] Other scientists have stated that the conclusion that the negative effects of back sleep at 18 months of age is transient is based upon very little evidence and that no long-term randomized trials have been completed.[76]
Other side effects of the back sleeping position include increased rates of shoulder retraction, positional plagiocephaly, and positional torticollis.[77] Some scientists dispute that plagiocephaly is a negative side effect. Dr. Peter Fleming, who is co-author of the study that deemed delays at 6 months of age to be transient, has stated that he does not think plagiocephaly is a negative side effect of back sleep. In an interview with the Guardian Dr. Fleming stated "I do not think it is a medical problem—it is more of a cosmetic one. Mothers may feel it is a syndrome and a problem when it really is nonsense."[78] A research study on children with plagiocephaly plus a confounding condition such as premature birth or failure to thrive, found that 26% had mild to severe psychomotor delay. This study also showed that 10% of infants with plagiocephaly had mild to severe mental development delay.[79]
Because of the delays caused by back sleep some medical professionals have suggested that the "normal" ages at which children had previously attained developmental milestones should be pushed back. This would enable medical professionals to consider "normal" children who previously were considered developmentally delayed.[80]
Additional studies have reported that the following negative conditions are associated with the back sleep position: increase in sleep apnea, decrease in sleep duration, strabismus, social skills delays, deformational plagiocephaly, and temporomandibular jaw difficulties.[77] In addition, the following are symptoms that are associated with sleep apnea: growth abnormalities, failure to thrive syndrome in infants, neurocognitive abnormalities, daytime sleepiness, emotional problems, decrease in memory, decrease in learning, and a delay in nonverbal skills. The conditions associated with deformational plagiocephaly include visual impairments, cerebral dysfunction, delays in psychomotor development and decreases in mental functioning. The conditions associated with gross motor milestone delays include speech and language disorders. In addition, it has been hypothesized that delays in motor skills can have a negative impact on the development of social skills.[81][82] In addition, other studies have reported that the prone position prevents subluxation of the hips, increases psychomotor development, prevents scoliosis, lessens the risk of gastroesophageal reflux, decreases infant screaming periods, causes less fatigue in infants, and increases the relief of infant colic.[83] In addition, prior to the "Back to Sleep" campaign many babies self-treated their own torticollis by turning their heads from one side to the other while sleeping in the prone position.[84] Supine sleeping infants cannot self-treat their own torticollis. jm
Pacifiers
According to a 2005 meta-analysis, most studies favor pacifier use.[6] According to the American Academy of Pediatrics, pacifier use seems to reduce the risk of SIDS, although the mechanism by which this happens is unclear.[85] SIDS experts and policy makers haven't recommended the use of pacifiers to reduce the risk of SIDS because of several problems associated with pacifier use, like increased risk of otitis, gastrointestinal infections and oral colonization with Candida species.[85] A 2005 study indicated that use of a pacifier is associated with up to a 90% reduction in the risk of SIDS depending on the ambient factors, and it reduced the effect of other risk factors.[86] It has been speculated that the raised surface of the pacifier holds the infant's face away from the mattress, reducing the risk of suffocation. If a postmortem investigation does not occur or is insufficient, a suffocated baby may be misdiagnosed with SIDS.
A 2010 study at Monash University suggests pacifiers can prevent SIDS by changing sleep patterns. They believe a pacifier ensures the baby remains in a light sleep and is more easily aroused if they feel uncomfortable.[87] The most recent 2011 study confirms that pacifier usage also reduces SIDS risks from other known SIDS risk factors [88]
Secondhand smoke reduction
According to the US Surgeon General's Report, secondhand smoke is connected to SIDS.[89] Infants who die from SIDS tend to have higher concentrations of nicotine and cotinine (a biological marker for secondhand smoke exposure) in their body fluids than those who die from other causes.[90] Parents who smoke can significantly reduce their children's risk of SIDS by either quitting or smoking only outside and leaving their house completely smoke-free.
The maternal pregnancy smoking rate decreased by 38% between 1990 and 2002.[91]
Sleep positioning
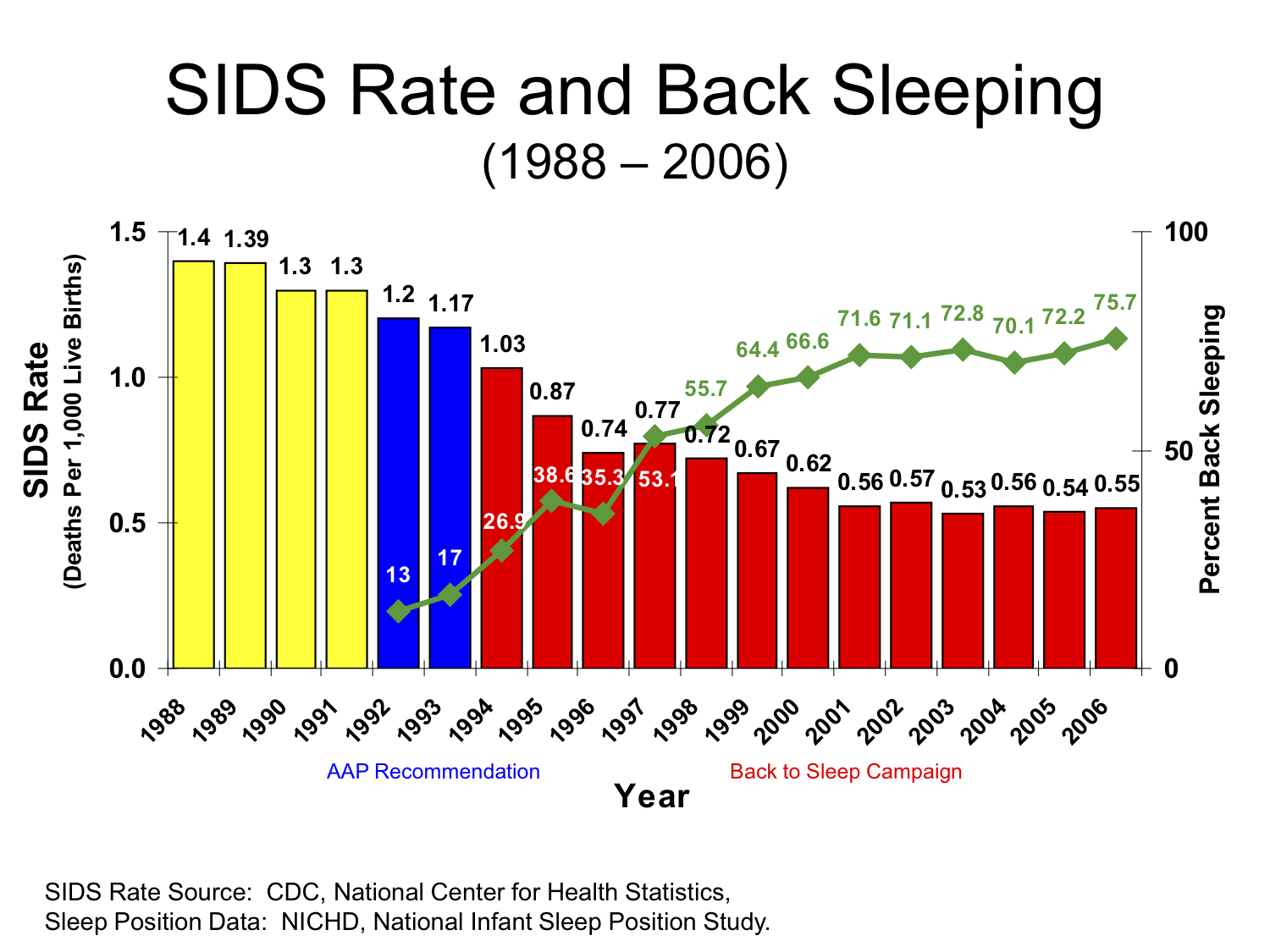
Main article: Back to Sleep A plot of SIDS rate from 1988 to 2006
A plot of SIDS rate from 1988 to 2006
Sleeping on the back has been recommended by (among others) the American Academy of Pediatrics (starting in 1992) to avoid SIDS, with the catchphrases "Back To Bed" and "Back to Sleep". The incidence of SIDS has fallen sharply in a number of countries in which the back to bed recommendation has been widely adopted, such as the US and New Zealand.[92] However, the absolute incidence of SIDS prior to the Back to Sleep Campaign was already dropping in the US, from 1.511 per 1000 in 1979 to 1.301 per 1000 in 1991.[13][original research?]
Among the theories supporting the Back to Sleep recommendation is the idea that small infants with little or no control of their heads may, while face down, inhale their exhaled breath (high in carbon dioxide) or smother themselves on their bedding—the brain-stem anomaly research (above) suggests that babies with that particular genetic makeup do not react "normally" by moving away from the pooled CO2, and thus smother. Another theory[93] is that babies sleep more soundly when placed on their stomachs, and are unable to rouse themselves when they have an incidence of sleep apnea, which is thought to be common in infants.
Hospital neonatal-intensive-care-unit (NICU) staff commonly place preterm newborns on their stomach, although they advise parents to place their infants on their backs after going home from the hospital.[94]
Sleep sacks
In colder environments where bedding is required to maintain a baby's body temperature, the use of a "baby sleep bag" or "sleep sack" is becoming more popular. This is a soft bag with holes for the baby's arms and head. A zipper allows the bag to be closed around the baby. A study published in the European Journal of Pediatrics in August 1998[95] has shown the protective effects of a sleep sack as reducing the incidence of turning from back to front during sleep, reinforcing putting a baby to sleep on its back for placement into the sleep sack and preventing bedding from coming up over the face which leads to increased temperature and carbon dioxide rebreathing. They conclude in their study "The use of a sleeping-sack should be particularly promoted for infants with a low birth weight." The American Academy of Pediatrics also recommends them as a type of bedding that warms the baby without covering its head.[96]
Epidemiology
SIDS was responsible for 0.543 deaths per 1,000 live births in the US in 2005.[13][original research?] It is responsible for far fewer deaths than congenital disorders and disorders related to short gestation, though it is the leading cause of death in healthy infants after one month of age.
SIDS deaths in the US decreased from 4,895 in 1992 to 2,247 in 2004.[97] But, during a similar time period, 1989 to 2004, SIDS being listed as the cause of death for sudden infant death (SID) decreased from 80% to 55%.[97] According to Dr. John Kattwinkel, chairman of the Centers for Disease Control and Prevention (CDC) Special Task Force on SIDS "A lot of us are concerned that the rate (of SIDS) isn't decreasing significantly, but that a lot of it is just code shifting".[97]
A set of 14 epidemiologic characteristics associated with SIDS have been identified:[98][99]
- A characteristic 4-parameter lognormal age distribution;
- Increased risk associated with prone sleep position;
- Prone and supine SIDS have same age and gender distributions;
- Male and female SIDS have same age distribution;
- Total sudden respiratory deaths at home have same age and gender distributions;[100]
- No evidence of cause of death at forensic autopsy and death scene investigation;
- SIDS spares infants at birth[?];
- Seasonality: winter maximum, summer minimum;
- Increasing SIDS rate with Live Birth Order;
- Consistent male excess of approximately 50%;
- Low increased risk of SIDS in subsequent siblings of SIDS;
- Parental smoking is a risk factor for SIDS;
- Acute Life Threatening Events (ALTE) are not a risk factor for subsequent SIDS;
- SIDS risk is greatest during sleep.
References
- ^ a b Glatt, John (2000). Cradle of Death: A Shocking True Story of a Mother, Multiple Murder, and SIDS. Macmillan. ISBN 0312973020.
- ^ a b Havill, Adrian (2002). While Innocents Slept: A Story of Revenge, Murder, and SIDS. Macmillan. ISBN 0312975171.
- ^ a b See CDC WONDER online database and http://www3.who.int/whosis/menu.cfm?path=whosis,inds,mort&language=english for data on SIDS by gender in the US and throughout the world.
- ^ a b Mage DT, Donner EM (September 2004). "The fifty percent male excess of infant respiratory mortality". Acta Paediatr. 93 (9): 1210–5. doi:10.1080/08035250410031305. PMID 15384886. http://www3.interscience.wiley.com/resolve/openurl?genre=article&sid=nlm:pubmed&issn=0803-5253&date=2004&volume=93&issue=9&spage=1210.
- ^ a b Coleman-Phox K, Odouli R, Li DK (October 2008). "Use of a fan during sleep and the risk of sudden infant death syndrome". Arch Pediatr Adolesc Med 162 (10): 963–8. doi:10.1001/archpedi.162.10.963. PMID 18838649. http://archpedi.ama-assn.org/cgi/content/abstract/162/10/963.
- ^ a b "Fig 4. Meta-analysis of studies examining the relationship of a pacifier used during the last sleep in SIDS victims versus controls". American Academy of Pediatrics. http://aappolicy.aappublications.org/cgi/content/full/pediatrics;116/5/1245/F4. Retrieved 2008-11-06.
- ^ Health Canada SIDS Healthy Babies SIDS Page.
- ^ NZ Ministry of Health
- ^ http://www.cdc.gov/SIDS/SUID.htm
- ^ a b c d Sullivan FM, Barlow SM. (2001). "Review of risk factors for Sudden Infant Death Syndrome". Paediatric Perinatal Epidemiology 15 (2): 144–200. doi:10.1046/j.1365-3016.2001.00330.x. PMID 11383580.
- ^ Lavezzi AM, Corna MF, Matturri L (July 2010). "Ependymal alterations in sudden intrauterine unexplained death and sudden infant death syndrome: possible primary consequence of prenatal exposure to cigarette smoking". Neural Dev 19 (5): 17. doi:10.1186/1749-8104-5-17. PMC 2919533. PMID 20642831. http://www.neuraldevelopment.com/content/5//17.
- ^ Weinberg ED (June 2000). "Association of primary Pneumocystis carinii infection and sudden infant death syndrome". Clin. Infect. Dis. 30 (6): 991. doi:10.1086/313796. PMID 10880335. http://www.journals.uchicago.edu/cgi-bin/resolve?CID000127.
- ^ a b c d e f CDC WONDER online database
- ^ Hunt CE (November 2007). "Small for gestational age infants and sudden infant death syndrome: a confluence of complex conditions". Arch. Dis. Child. Fetal Neonatal Ed. 92 (6): F428–9. doi:10.1136/adc.2006.112243. PMC 2675383. PMID 17951549. http://fn.bmj.com/cgi/pmidlookup?view=long&pmid=17951549.
- ^ Office of the Surgeon General of the United States Report on Involuntary Exposure to Tobacco Smoke (PDF)
- ^ Willinger M, Hoffman HJ, Hartford RB (May 1994). "Infant sleep position and risk for sudden infant death syndrome: report of meeting held January 13 and 14, 1994, National Institutes of Health, Bethesda, MD". Pediatrics 93 (5): 814–9. PMID 8165085.
- ^ "Secret to SIDS unlocked by researchers". Sydney Morning Herald. 21 October 2010. http://www.smh.com.au/lifestyle/wellbeing/secret-to-sids-unlocked-by-researchers-20101021-16vax.html. Retrieved 21 October 2010.
- ^ McKenna JJ, McDade T (June 2005). "Why babies should never sleep alone: a review of the co-sleeping controversy in relation to SIDS, bedsharing and breast feeding". Paediatr Respir Rev 6 (2): 134–52. doi:10.1016/j.prrv.2005.03.006. PMID 15911459. http://linkinghub.elsevier.com/retrieve/pii/S1526054205000230.
- ^ Moon RY, Horne RS, Hauck FR (November 2007). "Sudden infant death syndrome". Lancet 370 (9598): 1578–87. doi:10.1016/S0140-6736(07)61662-6. PMID 17980736.
- ^ Fleming PJ, Levine MR, Azaz Y, Wigfield R, Stewart AJ (June 1993). "Interactions between thermoregulation and the control of respiration in infants: possible relationship to sudden infant death". Acta Paediatr Suppl 82 (Suppl 389): 57–9. doi:10.1111/j.1651-2227.1993.tb12878.x. PMID 8374195.
- ^ McIntosh CG, Tonkin SL, Gunn AJ (2009). "What is the mechanism of sudden infant deaths associated with co-sleeping?". N. Z. Med. J. 122 (1307): 69–75. PMID 20148046.
- ^ Mage DT (1996). "A probability model for the age distribution of SIDS". J Sudden Infant Death Syndrome Infant Mortal 1: 13–31.
- ^ Poets CF, Samuels MP, Wardrop CA, Picton-Jones E, Southall DP (April 1992). "Reduced haemoglobin levels in infants presenting with apparent life-threatening events—a retrospective investigation". Acta Paediatr. 81 (4): 319–21. doi:10.1111/j.1651-2227.1992.tb12234.x. PMID 1606392.
- ^ Giulian GG, Gilbert EF, Moss RL (April 1987). "Elevated fetal hemoglobin levels in sudden infant death syndrome". N Engl J Med 316 (18): 1122–6. doi:10.1056/NEJM198704303161804. PMID 2437454.
- ^ Weber, M.; Klein, N.; Hartley, J.; Lock, P.; Malone, M.; Sebire, N. (2008). "Infection and sudden unexpected death in infancy: a systematic retrospective case review". The Lancet 371 (9627): 1848. doi:10.1016/S0140-6736(08)60798-9. PMID 18514728.
- ^ Task Force on Sudden Infant Death Syndrome (November 2005). "The changing concept of sudden infant death syndrome: diagnostic coding shifts, controversies regarding the sleeping environment, and new variables to consider in reducing risk". Pediatrics 116 (5): 1245–55. doi:10.1542/peds.2005-1499. PMID 16216901. http://aappolicy.aappublications.org/cgi/content/full/pediatrics;116/5/1245.
- ^ Ball H (September 2009). "Airway covering during bed-sharing". Child Care Health Dev 35 (5): 728–37. doi:10.1111/j.1365-2214.2009.00979.x. PMID 19531119. http://www3.interscience.wiley.com/resolve/openurl?genre=article&sid=nlm:pubmed&issn=0305-1862&date=2009&volume=35&issue=5&spage=728.
- ^ a b Paterson DS, Trachtenberg FL, Thompson EG, et al. (November 2006). "Multiple serotonergic brainstem abnormalities in sudden infant death syndrome". JAMA 296 (17): 2124–32. doi:10.1001/jama.296.17.2124. PMID 17077377.
- ^ a b Duncan JR, Paterson DS, Hoffman JM, Mokler DJ, Borenstein NS, Belliveau RA, Krous HF, Haas EA, Stanley C, Nattie EE, Trachtenberg FL, Kinney HC. Brainstem serotonergic deficiency in sudden infant death syndrome.JAMA. 2010 Feb 3;303(5):430-7.
- ^ Maggio AB, Schäppi MG, Benkebil F, Posfay-Barbe KM, Belli DC (November 2006). "Increased incidence of apparently life-threatening events due to supine position". Paediatric and Perinatal Epidemiology 20 (6): 491–6; discussion 496–7. doi:10.1111/j.1365-3016.2006.00753.x. PMID 17052284.
- ^ Kadhim H, Deltenre P, De Prez C, Sébire G. (August 2010). "Interleukin-2 as a neuromodulator possibly implicated in the physiopathology of sudden infant death syndrome". FNeurosci Lett. 480 (2): 122–6. doi:10.1016/j.neulet.2010.06.021. PMID 20542085.
- ^ Katz DM (2005). "Regulation of respiratory neuron development by neurotrophic and transcriptional signaling mechanisms". Respiratory physiology & neurobiology 149 (1–3): 99–109. doi:10.1016/j.resp.2005.02.007. PMID 16203214.
- ^ ICPA — SIDS Research
- ^ Spinelli, Margaret (2003). Infanticide: Psychosocial and Legal Perspectives on Mothers Who Kill. American Psychiatric Pub. p. 27. ISBN 1585620971.
- ^ Stanton J, Simpson A (December 2001). "Murder misdiagnosed as SIDS: a perpetrator's perspective". Arch Dis Child. 85 (6): 454–9. doi:10.1136/adc.85.6.454. PMC 1719021. PMID 11719326. http://adc.bmj.com/cgi/pmidlookup?view=long&pmid=11719326.
- ^ Emery JL (October 1993). "Child abuse, sudden infant death syndrome, and unexpected infant death". Am J Dis Child. 147 (10): 1097–100. PMID 8213682.
- ^ "Investigation of SIDS". N Engl J Med. 315 (26): 1675–7. December 1986. doi:10.1056/NEJM198612253152611. PMID 3785340.
- ^ Carol Strickland (1997-10-19). "Investigating a Rash of SIDS Deaths, Exposing Infanticide". The New York Times. http://query.nytimes.com/gst/fullpage.html?sec=health&res=9A06EED9163FF93AA25753C1A961958260. Retrieved 2008-04-20.
- ^ "Sir Roy Meadow struck off by GMC". BBC News. 2005-07-15. http://news.bbc.co.uk/1/hi/health/4685511.stm.
- ^ "About Statistics and the Law" (Website). Royal Statistical Society. (2001-10-23) Retrieved on 2007-09-22
- ^ See the data found at http://wonder.cdc.gov for 9ICD 911–912 and 10ICD W79-W80 for death rates from inhalation of food and foreign objects by sex.
- ^ Osmond C, Murphy M (October 1988). "Seasonality in the sudden infant death syndrome". Paediatr Perinat Epidemiol 2 (4): 337–45. doi:10.1111/j.1365-3016.1988.tb00228.x. PMID 3072532.
- ^ Thomas H. Maugh II (2007) (– Scholar search). Hearing loss may foretell SIDS risk. Los Angeles Times. http://www.latimes.com/news/science/la-sci-sids28jul28,1,2214491.story?track=rss.[dead link]
- ^ Alastruey J, Sherwin SJ, Parker KH, Rubens DD (January 2010). "Reply to 'Cord clamp insult may predispose to SIDS'". Early Human Development 86 (1): 67. doi:10.1016/j.earlhumdev.2009.12.002. PMID 20071109.
- ^ Alastruey J, Sherwin SJ, Parker KH, Rubens DD (July 2009). "Placental transfusion insult in the predisposition for SIDS: a mathematical study". Early Hum. Dev. 85 (7): 455–9. doi:10.1016/j.earlhumdev.2009.04.001. PMID 19446412. http://linkinghub.elsevier.com/retrieve/pii/S0378-3782(09)00060-7.
- ^ Klonoff-Cohen H, Lam PK, Lewis A (July 2005). "Outdoor carbon monoxide, nitrogen dioxide, and sudden infant death syndrome". Arch Dis Child. 90 (7): 750–3. doi:10.1136/adc.2004.057091. PMC 1720470. PMID 15970620. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1720470.
- ^ Fleming PJ, Blair PS, Mitchell EA (November 2002). "Mattresses, microenvironments, and multivariate analyses". BMJ 325 (7371): 981–2. doi:10.1136/bmj.325.7371.981. PMC 1124537. PMID 12411332. http://bmj.com/cgi/pmidlookup?view=long&pmid=12411332.
- ^ "Cot Life 2000 aims to eliminate cot". Cotlife2000.co.nz. http://www.cotlife2000.co.nz/. Retrieved 2009-10-15.
- ^ See FSID Press release.
- ^ cotlife2000.co.nz Errors and fallacies in the UK Limerick Report: an overview, Cot Life 2000
- ^ Vennemann MM, Butterfass-Bahloul T, Jorch G, et al. (January 2007). "Sudden infant death syndrome: no increased risk after immunisation". Vaccine 25 (2): 336–40. doi:10.1016/j.vaccine.2006.07.027. PMID 16945457.
- ^ a b Sudden Infant Death Syndrome (SIDS) and Vaccines http://www.cdc.gov/vaccinesafety/Concerns/sids_faq.html
- ^ Kalokerinos A, Dettman G (July 1976). "Sudden death in infancy syndrome in Western Australia". Med. J. Aust. 2 (1): 31–2. PMID 979792.
- ^ Donovan J (September 1979). "Vitamin C and cot death: where is the evidence?". Med. J. Aust. 2 (6): 311. PMID 522763.
- ^ Holborow P (April 1980). "Sudden infant death syndrome". Am. J. Clin. Nutr. 33 (4): 730–1. PMID 7361687. http://www.ajcn.org/cgi/reprint/33/4/730. "There has been some controversy about the role of Vitamin C in cot death."
- ^ Cheraskin E (October 1995). "Vitamin C, smoking and SIDS". J R Soc Health 115 (5): 332. doi:10.1177/146642409511500519. PMID 7473510.
- ^ Dick A, Ford R (November 2009). "Cholinergic and oxidative stress mechanisms in sudden infant death syndrome". Acta Paediatr. 98 (11): 1768–75. doi:10.1111/j.1651-2227.2009.01476.x. PMC 2773533. PMID 19706020. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2773533.
- ^ Yang Z, Lantz PE, Ibdah JA (December 2007). "Post-mortem analysis for two prevalent beta-oxidation mutations in sudden infant death". Pediatr Int 49 (6): 883–7. doi:10.1111/j.1442-200X.2007.02478.x. PMID 18045290. http://www3.interscience.wiley.com/resolve/openurl?genre=article&sid=nlm:pubmed&issn=1328-8067&date=2007&volume=49&issue=6&spage=883.
- ^ Nevas M, Lindström M, Virtanen A, et al. (January 2005). "Infant botulism acquired from household dust presenting as sudden infant death syndrome". J. Clin. Microbiol. 43 (1): 511–3. doi:10.1128/JCM.43.1.511-513.2005. PMC 540168. PMID 15635031. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=540168.
- ^ Millat G, Kugener B, Chevalier P, et al. (May 2009). "Contribution of long-QT syndrome genetic variants in sudden infant death syndrome". Pediatr Cardiol 30 (4): 502–9. doi:10.1007/s00246-009-9417-2. PMID 19322600.
- ^ Stray-Pedersen A, Vege A, Rognum TO (October 2008). "Helicobacter pylori antigen in stool is associated with SIDS and sudden infant deaths due to infectious disease". Pediatr. Res. 64 (4): 405–10. doi:10.1203/PDR.0b013e31818095f7. PMID 18535491. http://meta.wkhealth.com/pt/pt-core/template-journal/lwwgateway/media/landingpage.htm?issn=0031-3998&volume=64&issue=4&spage=405.
- ^ Bajanowski T, Vennemann M, Bohnert M, Rauch E, Brinkmann B, Mitchell EA (July 2005). "Unnatural causes of sudden unexpected deaths initially thought to be sudden infant death syndrome". Int. J. Legal Med. 119 (4): 213–6. doi:10.1007/s00414-005-0538-8. PMID 15830244.
- ^ Du Chesne A, Bajanowski T, Brinkmann B (1997). "[Homicides without clues in children]" (in German). Arch Kriminol 199 (1–2): 21–6. PMID 9157833.
- ^ Williams, FL; Lang, GA; Mage, DT (2001). "Sudden unexpected infant deaths in Dundee, 1882-1891: overlying or SIDS?". Scottish medical journal 46 (2): 43–7. PMID 11394337.
- ^ http://www.charlotteobserver.com/sids/
- ^ Carla K. Johnson (Associated Press writer) (2008-09-08). "Fan use linked to lower risk of sudden baby death". Toronto Star. http://www.parentcentral.ca/parent/article/513143. Retrieved 2008-11-09., also in Live Science
- ^ Vanderford J, Olsson J (May 2009). "Should we really encourage fan use?". Arch Pediatr Adolesc Med 163 (5): 490; author reply 490–1. doi:10.1001/archpediatrics.2009.79. PMID 19414701. http://archpedi.ama-assn.org/cgi/content/full/163/5/490.
- ^ Smartmoney.com on bedding
- ^ "What Can Be Done?". American SIDS Institute. http://www.sids.org/nprevent.htm.
- ^ Mitchell, E.; Thompson, J.; Becroft, D.; Bajanowski, T.; Brinkmann, B.; Happe, A.; Jorch, G.; Blair, P. et al. (2008). "Head covering and the risk for SIDS: findings from the New Zealand and German SIDS case-control studies". Pediatrics 121 (6): e1478–e1483. doi:10.1542/peds.2007-2749. PMID 18519451.
- ^ Hauck FR, Herman SM, Donovan M, Iyasu S, Merrick Moore C, Donoghue E, Kirschner RH, Willinger M (2003). "Sleep environment and the risk of sudden infant death syndrome in an urban population: the Chicago Infant Mortality Study". Pediatrics 111 (5 Part 2): 1207–14. PMID 12728140. http://pediatrics.aappublications.org/cgi/content/abstract/111/5/S1/1207.
- ^ Vennemann MM, Bajanowski T, Brinkmann B, et al. (March 2009). "Does breastfeeding reduce the risk of sudden infant death syndrome?". Pediatrics 123 (3): e406–10. doi:10.1542/peds.2008-2145. PMID 19254976. http://pediatrics.aappublications.org/cgi/pmidlookup?view=long&pmid=19254976.
- ^ "Policy Statement for Bumper Pads in Cribs — Consumer Product Safety". http://www.hc-sc.gc.ca/cps-spc/legislation/pol/bumper-bordure_e.html. Retrieved 2007-06-27.
- ^ Pelayo R, Owens J, Mindell J, Sheldon S (March 2006). "Bed sharing with unimpaired parents is not an important risk for sudden infant death syndrome: to the editor". Pediatrics 117 (3): 993–4; author reply 994–6. doi:10.1542/peds.2005-2748. PMID 16510694. http://pediatrics.aappublications.org/cgi/reprint/117/3/993.pdf.
- ^ Dewey C, Fleming P, Golding J (January 1998). "Does the supine sleeping position have any adverse effects on the child? II. Development in the first 18 months.ALSPAC Study Team". Pediatrics 101 (1): E5. doi:10.1542/peds.101.1.e5. PMID 9417169. http://pediatrics.aappublications.org/cgi/pmidlookup?view=long&pmid=9417169.
- ^ Pelligra R, Doman G, Leisman G (July 2005). "A reassessment of the SIDS Back to Sleep Campaign". Scientific World Journal 5: 550–7. doi:10.1100/tsw.2005.71. PMID 16075152. http://cgi.thescientificworld.co.uk/cgi-bin/processHtml.pl?Id=2005.03.71.html&format=Dreamweaver.[dead link]
- ^ a b Jones MW (2004). "Supine and Prone Infant Positioning: A Winning Combination". J Perinat Educ 13 (1): 10–20. doi:10.1624/105812404826388. PMC 1595182. PMID 17273371. http://www.ingentaconnect.com/content/springer/jpe/2004/00000013/00000001/art00006.
- ^ Carter H (July 8, 2003). "Flat Out". The Guardian.
- ^ Kordestani RK, Patel S, Bard DE, Gurwitch R, Panchal J (January 2006). "Neurodevelopmental delays in children with deformational plagiocephaly". Plast Reconstr Surg. 117 (1): 207–18; discussion 219–20. doi:10.1097/01.prs.0000185604.15606.e5. PMID 16404269. http://meta.wkhealth.com/pt/pt-core/template-journal/lwwgateway/media/landingpage.htm?an=00006534-200601000-00032.
- ^ Stevens P, "The Flip Side of Back to Sleep", The O&P Edge.
- ^ von Hofsten C (June 2004). "An action perspective on motor development". Trends Cogn. Sci. (Regul. Ed.) 8 (6): 266–72. doi:10.1016/j.tics.2004.04.002. PMID 15165552. http://linkinghub.elsevier.com/retrieve/pii/S1364661304001019.
- ^ Sigmundsson H, Haga M (October 2000). "[Children and motor competence]" (in Norwegian). Tidsskr. Nor. Laegeforen. 120 (25): 3048–50. PMID 11109395.
- ^ Högberg U, Bergström E (April 2000). "Suffocated prone: the iatrogenic tragedy of SIDS". Am J Public Health 90 (4): 527–31. doi:10.2105/AJPH.90.4.527. PMC 1446204. PMID 10754964. http://www.ajph.org/cgi/pmidlookup?view=long&pmid=10754964.
- ^ Graham JM, Gomez M, Halberg A, et al. (February 2005). "Management of deformational plagiocephaly: repositioning versus orthotic therapy". J. Pediatr. 146 (2): 258–62. doi:10.1016/j.jpeds.2004.10.016. PMID 15689920.
- ^ a b "The Changing Concept of Sudden Infant Death Syndrome: Diagnostic Coding Shifts, Controversies Regarding the Sleeping Environment, and New Variables to Consider in Reducing Risk". American Academy of Pediatrics. http://aappolicy.aappublications.org/cgi/content/full/pediatrics;116/5/1245#SEC6. Retrieved 2008-11-06.
- ^ Li DK, Willinger M, Petitti DB, Odouli R, Liu L, Hoffman HJ (2006). "Use of a dummy (pacifier) during sleep and risk of sudden infant death syndrome (SIDS): population based case-control study". BMJ 332 (7532): 18–22. doi:10.1136/bmj.38671.640475.55. PMC 1325127. PMID 16339767. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1325127.
- ^ "Dummies may protect babies babies from cot death". Sydney Morning Herald. 8 October 2010. http://www.smh.com.au/lifestyle/wellbeing/dummies-may-protect-babies-from-cot-death-20101007-169we.html. Retrieved 12 October 2010.
- ^ Moon RY, Tanabe KO, Yang DC, Young HA, Hauck FR (April 2011). "Pacifier Use and Sids: Evidence for a Consistently Reduced Risk". Matern Child Health J. doi:10.1007/s10995-011-0793-x. PMID 21505778.
- ^ Chapter 5; pages 180–194, secondhand smoke is connected to SIDS.
- ^ Bajanowski, T.; Brinkmann, B.; Mitchell, E.; Vennemann, M.; Leukel, H.; Larsch, K.; Beike, J.; Gesid, G. (2008). "Nicotine and cotinine in infants dying from sudden infant death syndrome". International journal of legal medicine 122 (1): 23–28. doi:10.1007/s00414-007-0155-9. PMID 17285322.
- ^ Centers for Disease Control and Prevention (CDC) (October 2004). "Smoking during pregnancy—United States, 1990–2002". MMWR Morb Mortal Wkly Rep. 53 (39): 911–5. PMID 15470322. http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5339a1.htm.
- ^ Mitchell EA, Hutchison L, Stewart AW (July 2007). "The continuing decline in SIDS mortality". Arch Dis Child. 92 (7): 625–6. doi:10.1136/adc.2007.116194. PMC 2083749. PMID 17405855. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2083749.
- ^ Blyth, T; McKenzie, S (2003). "SIDS, smoking, and arousal thresholds: conclusions not supported by data". Archives of disease in childhood. Fetal and neonatal edition 88 (2): F162; author reply F162. doi:10.1136/fn.88.2.F162. PMC 1721504. PMID 12598514. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1721504.
- ^ Aris C, Stevens TP, Lemura C, et al. (October 2006). "NICU nurses' knowledge and discharge teaching related to infant sleep position and risk of SIDS". Adv Neonatal Care 6 (5): 281–94. doi:10.1016/j.adnc.2006.06.009. PMID 17045948.
"Erratum". Adv Neonatal Care 6 (6): 340. December 2006. doi:10.1016/j.adnc.2007.01.001. - ^ L'Hoir MP, Engelberts AC, van Well GT, et al. (1998). "Risk and preventive factors for cot death in The Netherlands, a low-incidence country". Eur. J. Pediatr. 157 (8): 681–8. doi:10.1007/s004310050911. PMID 9727856.
- ^ "The Changing Concept of Sudden Infant Death Syndrome: Diagnostic Coding Shifts, Controversies Regarding the Sleeping Environment, and New Variables to Consider in Reducing Risk". American Academy of Pediatrics. http://aappolicy.aappublications.org/cgi/content/full/pediatrics;116/5/1245#SEC15. Retrieved 2008-11-06.
- ^ a b c Bowman L, Hargrove T. Exposing Sudden Infant Death In America. Scripps Howard News Service. http://dailycamera.com/news/2007/oct/08/saving-babies-exposing-sudden-infant-death-in/
- ^ Mage DT, Donner EM (2004). "Is SIDS at Borkmann's Point?". Medical Hypotheses and Research 1 (2/3): 131–7.
- ^ Mage DT, Donner EM (2011). "The universal age distribution of the Sudden Infant Death Syndrome". Scandinavian Journal of Forensic Science 17 (1): 4–8.
- ^ Carpenter RG, Gardner A (1982). "Variations in unexpected infant death rates relating to age, sex and season". Studies on Medical and Population Subjects. 45. London: HMSO. pp. 23–31.
Further reading
- Ottaviani, G. (2007). Crib death. Sudden unexplained death of infants: the pathologist's viewpoint. Berlin Heidelberg, Germany: Springer. ISBN 978 3 540 49370 9.
- Joan Hodgman; Toke Hoppenbrouwers (2004). SIDS. Calabasas, Calif: Monte Nido Press. ISBN 0-9742663-0-2.
- Lewak N. "Book Review: SIDS". Arch Pediatr Adolesc Med 158 (4): 405. http://archpedi.highwire.org/cgi/content/full/158/4/405.
External links
- SIDS at the Open Directory Project
Categories:- Causes of death
- Ailments of unknown etiology
- Pediatrics
- Infancy
- Sleep
- Children and death
Wikimedia Foundation. 2010.