- Ebola
Taxobox
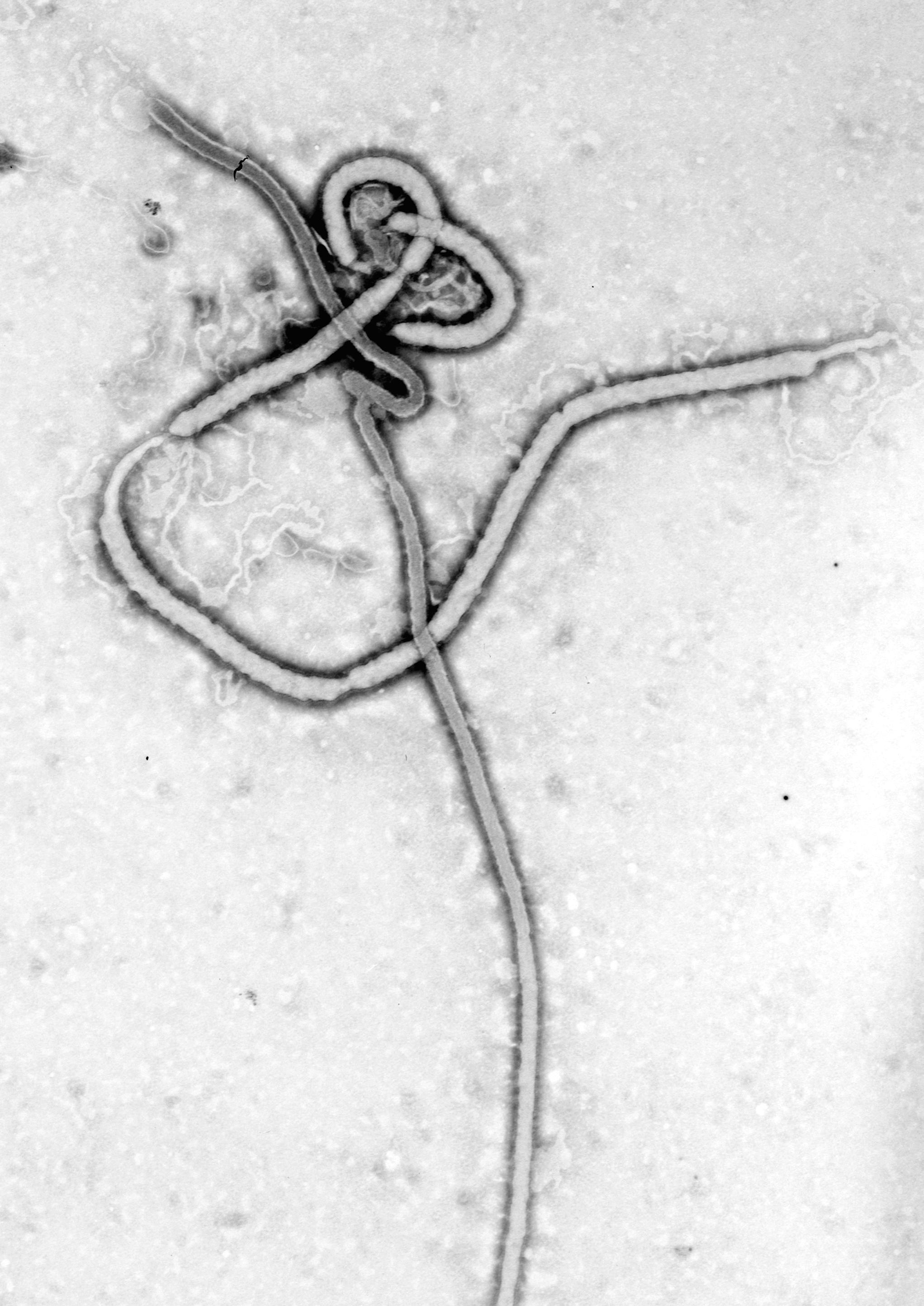
name = Ebola
image_width = 200px
image_caption = An electron micrograph of an Ebola virus
virus_group = V
ordo = "Mononegavirales "
familia = "Filovirus "
genus = "Ebolavirus"
type_species = "Zaïre ebolavirus"
subdivision_ranks = Species
subdivision = "Bundibugyo ebolavirus"
"Ivory Coast ebolavirus"
"Reston ebolavirus "
"Sudan ebolavirus"Infobox_Disease
Name = Ebola
Caption =
DiseasesDB = 18043
ICD10 = ICD10|A|98|4|a|90
ICD9 = ICD9|065.8
ICDO =
OMIM =
MedlinePlus = 001339
eMedicineSubj = medeMedicineTopic = 626
MeshName = Ebola
MeshNumber = C02.782.417.415Ebola is the common term for a group of
virus es belonging to genus "Ebolavirus", family "Filoviridae ", and for the disease which they cause, Ebola hemorrhagic fever. The virus is named after theEbola River where the first recognised outbreak of Ebola hemorrhagic fever occurred. The viruses are characterized by long filaments and have a similar shape to theMarburg virus , also in the family "Filoviridae", and share similar disease symptoms. Since its discovery, "Ebolavirus" has been responsible for a number of deaths.cite web | url = http://www.cdc.gov/ncidod/dvrd/spb/mnpages/dispages/ebotabl.htm | title = Ebola Cases and Outbreaks - CDC Special Pathogens Branch | accessdate = 2007-12-08 | author = | authorlink = | coauthors = | date = | format = | work = | publisher = Centers for Disease Control and Prevention]Overview
"Ebolavirus" first came to notice in 1976 in outbreaks of Ebola hemorrhagic fever in
Zaire andSudan . [cite journal |author=Bennett D, Brown D |title=Ebola virus |journal=BMJ |volume=310 |issue=6991 |pages=1344–5 |year=1995 |pmid=7787519 |doi= |url=http://www.bmj.com/cgi/content/full/310/6991/1344] The strain of Ebola which broke out in Zaire has one of the highestcase fatality rate s of any human pathogenic virus, roughly 90%. [cite web |url=http://www.emedicine.com/MED/topic626.htm |accessdate=2008-10-06 |author=King, John W |title=Ebola Virus |date=April 2, 2008 |work=eMedicine |publisher=WebMd] The strain which broke out later in Sudan has a case fatality rate of around 50%. [cite web |url=http://www.emedicine.com/MED/topic626.htm |accessdate=2008-10-06 |author=King, John W |title=Ebola Virus |date=April 2, 2008 |work=eMedicine |publisher=WebMd] The virus is believed to be transmitted to humans via contact with an infected animal host. The virus is then transmitted to other people who come into contact with infected blood and bodily fluids of the infected person, and by human contact with contaminated medical equipment such as needles. Both of these infectious mechanisms will occur in clinical (nosocomial ) and non-clinical situations. Due to the high fatality rate, the rapidity of demise, and the often remote areas where infections occur, the potential for widespreadepidemic outbreaks is considered low.Ebola is believed to be a zoonotic virus as it is currently devastating the populations of
Western Lowland Gorilla s inCentral Africa . As of late 2005, three species offruit bat have been identified as carrying the virus but not showing disease symptoms, and they are now believed to be the natural host species, or reservoir, of the virus.fact|date=August 2008Ebola hemorrhagic fever is potentially lethal and encompasses a range of symptoms including
fever ,vomiting ,diarrhea , generalized pain or malaise, and sometimes internal and external bleeding.Mortality rate s are extremely high, with the human case-fatality rate ranging from 50–89%, depending on viral subtype. [cite journal |author=Rouquet P, Froment JM, Bermejo M, "et al" |title=Wild animal mortality monitoring and human Ebola outbreaks, Gabon and Republic of Congo, 2001-2003 |journal=Emerging Infect. Dis. |volume=11 |issue=2 |pages=283–90 |year=2005 |pmid=15752448 |doi= |url=http://www.cdc.gov/ncidod/EID/vol11no02/04-0533.htm] The cause of death is usually due to hypovolemic shock or organ failure.Ebola is potentially lethal, and since no approved
vaccine or treatment is available, Ebola is classified as a biosafety level 4 agent, as well as a Category A bioterrorism agent by theCenters for Disease Control and Prevention . It has the potential to be weaponized for use inbiological warfare . [cite journal |author=Borio L, Inglesby T, Peters CJ, "et al" |title=Hemorrhagic fever viruses as biological weapons: medical and public health management |journal=JAMA |volume=287 |issue=18 |pages=2391–405 |year=2002 |pmid=11988060 |doi= |url=http://jama.ama-assn.org/cgi/pmidlookup?view=long&pmid=11988060] Its effectiveness as a biological-warfare agent is compromised by its extreme deadliness and its level of contagion: a typical outbreak spreads through a small village or hospital, infects the entire population, and then runs out of potential hosts, dying out before reaching the wider community. It is also significant that none of the strains of Ebola known to cause disease in humans have been found to be airborne—only the strain known as Ebola Reston (after the city ofReston, Virginia where it was first identified in Green Monkeys) is believed to be airborne.Etymology
The virus is named after the
Ebola River Valley in theDemocratic Republic of the Congo (formerly Zaïre), which is near the site of the first recognized outbreak in 1976, in a mission hospital run by Flemishnun s. [cite journal |last=Bardi |first=Jason Socrates |authorlink= |coauthors= |year=2002 |month= |title=Death Called a River |journal=Scripps Research Institute |volume=2 |issue=1 |pages= |id= |url=http://www.scripps.edu/newsandviews/e_20020114/ebola1.html |accessdate=2006-12-08 |quote= ]Virology
Size and shape
Electron micrographs of members of genus "Ebolavirus" show them to have the characteristic thread-like structure of a filovirus.cite book |title=Ebola and Marburg Viruses, Molecular and Cellular Biology |last=Klenk |first=Hans-Dieter |authorlink= |coauthors=Feldmann, Heinz |year=2004 |publisher=Horizon Bioscience |location=Wymondham, Norfolk |isbn=0954523237 |pages= ] EBOV VP30 is around 288 amino acids long. The virions are tubular in general form but variable in overall shape and may appear as the classic shepherd's crook or eyebolt, as a "U" or a "6", or coiled, circular, or branched. However, laboratory purification techniques such as
centrifugation may contribute to some of these. Virions are generally 80 nm in diameter. They are of variable length, typically around 1000 nm, but may be up to 1400 nm long. In the center of the virion is a structure called "nucleocapsid", which is formed by the helically wound viral genomic RNA complexed with the proteins NP, VP35, VP30 and L. It has a diameter of 40-50 nm and contains a central channel of 20–30 nm in diameter. Virally encodedglycoprotein (GP) spikes 10 nm long and 10 nm apart are present on the outerviral envelope of the virion, which is derived from the host cell membrane. Between envelope and nucleocapsid, in the so-called matrix space, the viral proteins VP40 and VP24 are located.Genome
Each virion contains one minor molecule of linear, single-stranded, negative-sense RNA, totaling 18,959 to 18,961 nucleotides in length. The 3′ terminus is not polyadenylated and the 5′ end is not capped. It was found that 472 nucleotides from the 3' end and 731 nucleotides from the 5' end were sufficient for replication. It codes for seven structural proteins and one non-structural protein. The gene order is 3′ - leader - NP - VP35 - VP40 - GP/sGP - VP30 - VP24 - L - trailer - 5′; with the leader and trailer being non-transcribed regions which carry important signals to control transcription, replication and packaging of the viral genomes into new virions. The genomic material by itself is not infectious, because viral proteins, among them the RNA-dependent RNA polymerase, are necessary to transcribe the viral genome into mRNAs, as well as for replication of the viral genome.
Life cycle
* Virus attaches to host receptors through the GP (glycoprotein) surface
peplomer and is endocytosed into vesicles in the host cell.* Fusion of virus membrane with the vesicle membrane occurs; nucleocapsid is released into the cytoplasm.
* The encapsidated, negative-sense genomic ssRNA is used as a template for the synthesis ( 3' - 5') of polyadenylated, monocistronic mRNAs.
* Translation of the mRNA into viral proteins occurs using the host cell's machinery.
* Post-translational processing of viral proteins occurs. GP0 (glycoprotein precursor) is cleaved to GP1 and GP2, which are heavily glycosylated. These two molecules assemble, first into heterodimers, and then into trimers to give the surface peplomers. SGP (secreted glycoprotein) precursor is cleaved to SGP and delta peptide, both of which are released from the cell.
* As viral protein levels rise, a switch occurs from translation to replication. Using the negative-sense genomic RNA as a template, a complementary +ssRNA is synthesized; this is then used as a template for the synthesis of new genomic (-)ssRNA, which is rapidly encapsidated.
* The newly formed nucleocapsides and envelope proteins associate at the host cell's plasma membrane; budding occurs, and the virions are released.
Viral reservoirs
Despite numerous studies, the wildlife reservoir of "Ebolavirus" has not been identified. Between 1976 and 1998, from 30,000 mammals, birds, reptiles, amphibians, and arthropods sampled from outbreak regions, no "Ebolavirus" was detectedcite journal |author=Pourrut X, Kumulungui B, Wittmann T, "et al" |title=The natural history of Ebola virus in Africa |journal=Microbes Infect. |volume=7 |issue=7-8 |pages=1005–14 |year=2005 |pmid=16002313 |doi=10.1016/j.micinf.2005.04.006 |url=http://linkinghub.elsevier.com/retrieve/pii/S1286-4579(05)00143-7] apart from some genetic material found in six rodents ("Mus setulosus" and "Praomys" species) and a
shrew ("Sylvisorex ollula") collected from theCentral African Republic in 1998.cite journal |author=Morvan JM, Deubel V, Gounon P, "et al" |title=Identification of Ebola virus sequences present as RNA or DNA in organs of terrestrial small mammals of the Central African Republic |journal=Microbes Infect. |volume=1 |issue=14 |pages=1193–201 |year=1999 |pmid=10580275 |doi=10.1016/S1286-4579(99)00242-7 |url=http://linkinghub.elsevier.com/retrieve/pii/S1286-4579(99)00242-7] "Ebolavirus" was detected in the carcasses ofgorilla s,chimpanzee s andduiker s during outbreaks in 2001 and 2003 (the carcasses were the source of the initial human infections), but the high mortality from infection in these species precludes them from acting as reservoirs.Plant s,arthropods , and birds have also been considered as reservoirs; however, bats are considered the most likely candidate. [cite news |first= |last= |authorlink= |coauthors= |title=Fruit bats may carry Ebola virus |url=http://news.bbc.co.uk/2/hi/health/4484494.stm |work=BBC News |publisher= |date=2005-12-11 |accessdate=2008-02-25 ] Bats were known to reside in the cotton factory in which the index cases for the 1976 and 1979 outbreaks were employed and have also been implicated in Marburg infections in 1975 and 1980. Of 24 plant species and 19 vertebrate species experimentally inoculated with "Ebolavirus", only bats became infected. [cite journal |author=Swanepoel R, Leman PA, Burt FJ,"et al" |title=Experimental inoculation of plants and animals with Ebola virus |journal=Emerging Infect. Dis. |volume=2 |issue=4 |pages=321–5 |year=1996 |pmid=8969248 |doi= |url=http://www.cdc.gov/ncidod/eid/vol2no4/swanepo2.htm] The absence of clinical signs in these bats is characteristic of a reservoir species. In 2002-03, a survey of 1,030 animals fromGabon and theRepublic of the Congo including 679 bats found "Ebolavirus" RNA in 13fruit bats ("Hyspignathus monstrosus", "Epomops franquetti" and "Myonycteris torquata"). [cite journal |author=Leroy EM, Kumulungui B, Pourrut X, "et al" |title=Fruit bats as reservoirs of Ebola virus |journal=Nature |volume=438 |issue=7068 |pages=575–6 |year=2005 |pmid=16319873 |doi=10.1038/438575a|url=] Bats are also known to be the reservoirs for a number of related viruses includingNipah virus ,Hendra virus andlyssavirus es.Subtypes
Microbiologists have defined several subtypes of Ebola. The following list is not exclusive. A new strain of "Ebolavirus" has been identified in Uganda during an outbreak. It does not match any of the four Ebola subtypes previously identified by scientists. [cite news |first= |last= |authorlink= |coauthors= |title=New subtype of Ebola suspected in Uganda |url=http://www.usatoday.com/news/world/2007-11-30-uganda-ebola_N.htm |work=
USA Today |publisher= |date=2007-11-30 |accessdate=2008-02-25 ]Zaïre ebolavirus
The "Zaïre ebolavirus" has the highest case fatality rate, up to 90% in some epidemics, with an average case fatality rate of approximately 83% over 27 years. The case-fatality rates were 88% in 1976, 100% in 1977, 59% in 1994, 81% in 1995, 73% in 1996, 80% in 2001-2002 and 90% in 2003. There have been more outbreaks of "Zaïre ebolavirus" than any other strain.
The first outbreak took place on
August 26 ,1976 , inYambuku , a town in the north of Zaïre. The first recorded case was Mabalo Lokela, a 44-year-old schoolteacher returning from a trip around the north of the state. His high fever was diagnosed as possiblemalaria and he was subsequently given aquinine shot. Lokela returned to the hospital every day. A week later, his symptoms included uncontrolledvomiting , bloody diarrhea,headache ,dizziness , and trouble breathing. Later, he began bleeding from his nose, mouth, and anus. Lokela died onSeptember 8 ,1976 , roughly 14 days after the onset of symptoms.Soon after, more patients arrived with varying but similar symptoms including fever, headache, muscle and joint aches, fatigue, nausea, and dizziness. These often progressed to bloody diarrhea, severe vomiting, and bleeding from the nose, mouth, and anus. The initial transmission was believed to be due to reuse of the needle for Lokela's injection without sterilization. Subsequent transmission was also due to care of the sick patients without barrier nursing and the traditional burial preparation method, which involved washing and
gastrointestinal tract cleansing.Two nuns working in Yambuku as nurses also died in the same outbreak. [cite paper |last=Isaacson |first=Margaretha |author= |authorlink= |coauthors="et al." |title=Two Belgian nurses died of Ebola |version= |publisher= |date= |url=http://www.itg.be/ebola/ebola-12.htm |format= |id= |accessdate= ]
Sudan ebolavirus
"Sudan ebolavirus" was the second strain of Ebola reported in 1976. It apparently originated amongst cotton factory workers in Nzara, Sudan. The first case reported was a worker exposed to a potential natural reservoir at the cotton factory. Scientists tested all animals and insects in response to this, however none tested positive for the virus. The carrier is still unknown.
A second case involved a nightclub owner in Nzara,
Sudan . The local hospital, Maridi, tested and attempted to treat the patient; however, nothing was successful, and he died. The hospital did not advocate safe and practical procedures in sterilizing and disinfecting the medical tools used on the nightclub owner, likely facilitating the spread of the virus in the hospital.The most recent outbreak of "Sudan ebolavirus" occurred in May 2004. As of May 2004, 20 cases of "Sudan ebolavirus" were reported in Yambio County,
Sudan , with five deaths resulting. TheCenters for Disease Control and Prevention confirmed the virus a few days later. The neighbouring countries ofUganda and theDemocratic Republic of Congo have increased surveillance in bordering areas, and other similar measures have been taken to control the outbreak. The average fatality rates for "Sudan ebolavirus" were 54% in 1976, 68% in 1979, and 53% in 2000/2001. The average case-fatality rate is 54%.Reston ebolavirus
The "Reston ebolavirus" is suspected of being either another subtype of the
Ebola or a new filovirus ofAsia n origin. It was discovered in crab-eating macaques from Hazleton Labortories (now Covance) in 1989. This discovery attracted significant media attention and led to the publication of "The Hot Zone ". Despite its status as a Level-4 organism, the "Reston ebolavirus" is non-pathogen ic to humans and is only mildly fatal to monkeys; ["Level 4: Virus Hunters of the CDC" (1999), p.300. Quotation: "While it is true that we could take only so much comfort from the fact that the Reston virus was not pathogenic for humans—that it did not make people sick—there was always the threat of yet another strain turning up in monkeys imported from somewhere else, which might prove harmful to humans."] the perception of its lethality was skewed due to the monkey'scoinfection withSimian hemorrhagic fever virus (SHFV)."Level 4: Virus Hunters of the CDC" (1999), ppgs.307-309.]During the incident in which it was discovered, six animal handlers eventually became
seroconverted , one of whom had cut himself while performing anecropsy on the liver of an infected monkey. When the handler failed to become ill, it was concluded that the virus had a very lowpathogen icity to humans. ["Level 4: Virus Hunters of the CDC" (1999), ppgs.298-299.] Monkeys infected with "Reston ebolavirus" were again shipped to Reston, as well as Alice,Texas , in February 1990. More cases of "Reston ebolavirus"-infected monkeys were discovered inSiena ,Italy in 1992, and in Texas again in March 1996.Tai (Ivory Coast) ebolavirus
This subtype of Ebola was first discovered amongst
chimpanzee s of the Tai Forest inCôte d'Ivoire ,Africa . OnNovember 1 ,1994 , the corpses of two chimpanzees were found in the forest. Necropsies showed blood within the heart to be liquid and brown, no obvious marks seen on the organs, and one with lungs filled with liquid blood. Studies of tissues taken from the chimps showed results similar to human cases during the 1976 Ebola outbreaks in Zaïre and Sudan. Later in 1994, more dead chimpanzees were discovered, with many testing positive to Ebola using molecular techniques. The source of contamination was believed to be the meat of infectedWestern Red Colobus monkeys, upon which the chimpanzees preyed. [ [http://virus.stanford.edu/filo/eboci.html Ebola Cote d'Ivoire Outbreaks ] ]One of the scientists performing the necropsies on the infected chimpanzees contracted Ebola. She developed symptoms similar to
dengue fever approximately a week after the necropsy and was transported to Switzerland for treatment. After two weeks she was discharged from hospital, and was fully recovered six weeks after the infection.Bundibugyo ebolavirus
On
November 24 ,2007 , theUganda Ministry of Health confirmed an outbreak of Ebola in theBundibugyo District . After confirmation of samples tested by theUnited States National Reference Laboratories and theCenters for Disease Control , theWorld Health Organization confirmed the presence of a new species of "Ebolavirus". OnFebruary 20 ,2008 , the Uganda Ministry officially announced the end of the epidemic in Bundibugyo with the last infected person discharged onJanuary 8 ,2008 . [cite press release |title=End of Ebola outbreak in Uganda |publisher=World Health Organization |date=2008-02-20 |url=http://www.who.int/csr/don/2007_02_20b/en/index.html |format= |language= |accessdate= |quote= ] Ugandan officials confirmed a total of 149 cases of this new Ebola species, with 37 deaths attributed to the strain. [cite news |first=Tim |last= Cocks|authorlink= |coauthors= |title=Uganda confirms 113 suspected Ebola cases |url=http://africa.reuters.com/top/news/usnBAN126612.html |work= |publisher=Reuters |date=2007-12-11 |accessdate=2008-02-25 ]Ebola hemorrhagic fever
Symptoms
Symptoms are varied and often appear suddenly. Initial symptoms include high
fever (at least 38.8°C; 101.8°F), severe headache, muscle, joint, orabdominal pain , severe weakness andexhaustion , sore throat,nausea , anddizziness . [http://www.who.int/csr/disease/ebola/en/ WHO Fact Sheet Ebola haemorrhagic fever] ] Before anoutbreak is suspected, these early symptoms are easily mistaken formalaria ,typhoid fever ,dysentery ,influenza , or various bacterial infections, which are all far more common and reliably less fatal.Ebola may progress to cause more serious symptoms, such as
diarrhea , dark or bloodyfeces , vomiting blood, red eyes due todistension and hemorrhage of sclerotic arterioles,petechia ,maculopapular rash , andpurpura . Other secondary symptoms includehypotension (lowblood pressure ),hypovolemia ,tachycardia , organ damage (especially thekidneys ,spleen , andliver ) as a result of disseminated systemicnecrosis , andproteinuria . The interior bleeding is caused by a reaction between the virus and theplatelets that produces a chemical that will cut cell-sized holes into the capillary walls. After 5–7 days the person will die of "a million cuts".Fact|date=August 2008Occasionally, internal and external hemorrhage from orifices, such as the nose and mouth, may also occur, as well as from incompletely healed injuries such as needle-puncture sites. Ebola virus can affect the levels of
white blood cells and platelets, disrupting clotting.Fact|date=May 2007 More than 50% of patients will develop some degree of hemorrhaging.Fact|date=August 2008Methods of diagnosis of Ebola include testing saliva and urine samples. The span of time from onset of symptoms to death is usually between 7 and 14 days. By the second week of infection, patients will either defervesce (the fever will lessen) or undergo systemic multi-organ failure. Mortality rates are generally high, ranging from 50 to 90%. The cause of death is usually due to hypovolemic shock or organ failure. [cite journal |author=Bray M, Geisbert TW |title=Ebola virus: the role of macrophages and dendritic cells in the pathogenesis of Ebola hemorrhagic fever |journal=Int. J. Biochem. Cell Biol. |volume=37 |issue=8 |pages=1560–6 |year=2005 |pmid=15896665 |doi=10.1016/j.biocel.2005.02.018 |url=http://linkinghub.elsevier.com/retrieve/pii/S1357-2725(05)00072-5]
Filoviruses replicate well in a wide range of organs and cell types such as hepatocytes, epithelial cells, fibroblasts, fibroblastic reticular cells and adrenal cortical cells. Most notably, the susceptibility of human
endothelial cells is likely the cause of the symptoms that appear in the late stages of the infection such as shock syndrome and hemorrhaging.Transmission
Among humans, the virus is transmitted by direct contact with infected
body fluid s or, to a lesser extent, skin ormucous membrane contact. Theincubation period can range from 2 to 21 days, but is generally 5–10 days.Although
airborne transmission between monkeys has been demonstrated by an accidental outbreak in a laboratory located in Virginia, USA, there is very limited evidence for human-to-human airborne transmission in any reported epidemics. Nurse Mayinga might represent the only possible case. The means by which she contracted the virus remains uncertain.The infection of human cases with "Ebolavirus" has been documented through the handling of infected chimpanzees, gorillas, and forest antelopes—both dead and alive—as was documented in Côte d'Ivoire, the Republic of Congo and Gabon. The transmission of the Ebola Reston strain through the handling of cynomolgus monkeys has also been reported.
So far, all epidemics of Ebola have occurred in sub-optimal hospital conditions, where practices of basic hygiene and sanitation are often either luxuries or unknown to caretakers and where disposable needles and
autoclave s are unavailable or too expensive. In modern hospitals with disposable needles and knowledge of basic hygiene and barrier nursing techniques, Ebola has never spread on such a large scale.In the early stages, Ebola may not be highly contagious. Contact with someone in early stages may not even transmit the disease. As the illness progresses, bodily fluids from diarrhea, vomiting, and bleeding represent an extreme
biohazard . Due to lack of proper equipment and hygienic practices, large scale epidemics occur mostly in poor, isolated areas without modern hospitals or well-educated medical staff. Many areas where the infectious reservoir exists have just these characteristics. In such environments, all that can be done is to immediately cease all needle-sharing or use without adequate sterilization procedures, to isolate patients, and to observe strict barrier nursing procedures with the use of a medical rated disposable face mask, gloves, goggles, and a gown at all times. This should be strictly enforced for all medical personnel and visitors.Ebola is unlikely to develop into a
pandemic , or world-wide infection, due to its difficulty in spreading byairborne transmission and the period of time that the virus can use a living and contagious victim to spread compared to other infectious diseases. In isolated settings such as a quarantined hospital or a remote village, most victims are infected shortly after the first case of infection is present. In addition, the quick onset of symptoms from the time the disease becomes contagious in an individual makes it easy to identify sick individuals and limits an individual's ability to spread the disease by traveling. Because bodies of the deceased are still infectious, some doctors had to take measures to make sure that the disposal of dead bodies were conducted in a safe manner despite any local traditional burial rituals.cite news |first=Blaine |last=Harden |authorlink= |coauthors= |title=Dr. Matthew's Passion |url=http://www.nytimes.com/library/magazine/home/20010218mag%2debola.html |work=New York Times Magazine |publisher= |date=2001-02-18 |accessdate=2008-02-25 ]Treatments
There is no standard treatment for Ebola HF. Treatment is primarily supportive and includes minimizing invasive procedures, balancing electrolytes since patients are frequently dehydrated, replacing lost
coagulation factor s to help stop bleeding, maintaining oxygen and blood levels, and treating any complicating infections. Convalescent plasma (factors from those who have survived Ebola infection) shows promise as a treatment for the disease Fact|date=April 2008. Ribavirin is ineffective.Interferon is also thought to be ineffective. In monkeys, administration of an inhibitor of coagulation (rNAPc2) has shown some benefit, protecting 33% of infected animals from a usually 100% (for monkeys) lethal infection (unfortunately, this inoculation does not work on humans). In early 2006, scientists atUSAMRIID announced a 75% recovery rate after infecting fourrhesus monkey s with "Ebolavirus" and administering antisense drugs. [cite press release |title=USAMRIID press release |publisher= |date= |url=http://www.usamriid.army.mil/press%20releases/warfield_press_release.pdf |format= |language= |accessdate= |quote= ]Vaccines
Vaccines have been produced for both Ebolacite journal |author=Jones SM, Feldmann H, Ströher U, "et al" |title=Live attenuated recombinant vaccine protects nonhuman primates against Ebola and Marburg viruses |journal=Nat. Med. |volume=11 |issue=7 |pages=786–90 |year=2005 |pmid=15937495 |doi=10.1038/nm1258 |url=] and Marburgcite journal |author=Hevey M, Negley D, Pushko P, Smith J, Schmaljohn A |title=Marburg virus vaccines based upon alphavirus replicons protect guinea pigs and nonhuman primates |journal=Virology |volume=251 |issue=1 |pages=28–37 |year=1998 |pmid=9813200 |doi=10.1006/viro.1998.9367 |url=http://linkinghub.elsevier.com/retrieve/pii/S0042-6822(98)99367-9] that were 99% effective in protecting a group of monkeys from the disease. These vaccines are based on either a recombinant
Vesicular stomatitis virus or a recombinant Adenoviruscite journal |author=Sullivan NJ, Geisbert TW, Geisbert JB, "et al" |title=Accelerated vaccination for Ebola virus haemorrhagic fever in non-human primates |journal=Nature |volume=424 |issue=6949 |pages=681–4 |year=2003 |pmid=12904795 |doi=10.1038/nature01876 |url=] carrying the Ebola spikeprotein on its surface. Early human vaccine efforts, like the one atNIAID in 2003, have so far not reported any successes. [cite press release |title=NIAID Ebola Vaccine Enters Human Trial |publisher=National Institute of Allergy and Infectious Diseases |date=2003-11-18 |url=http://www3.niaid.nih.gov/news/newsreleases/2003/ebolahumantrial.htm |format= |language= |accessdate= |quote= ] The biggest problem with the vaccine is that unless the patient is given it near the onset of the virus (1-4 days after the symptoms begin), then there will be too much damage to the human body to repair, e.g., ruptured arteries and capillaries, vomiting, and other symptoms which may still cause enough harm to kill or seriously traumatize the patient.Recent outbreaks
As of
August 30 ,2007 , 103 people (100 adults and three children) were infected by a suspected hemorrhagic fever outbreak in the village ofKampungu, Democratic Republic of the Congo (DRC). The outbreak started after the funerals of two village chiefs, and 217 people in four villages fell ill. TheWorld Health Organization sent a team to take blood samples for analysis and confirmed that many of the cases are the result of "Ebolavirus". [cite news |first= |last= |authorlink= |coauthors= |title=Ebola Outbreak Confirmed in Congo |url=http://www.newscientist.com/article/dn12624-ebola-outbreak-confirmed-in-congo.html |work=NewScientist.com |publisher= |date=2007-09-11 |accessdate = 2008-02-25 ] The Congo's last major Ebola epidemic killed 245 people in 1995 inKikwit , about 200 miles from the source of the August 2007 outbreak. [cite news |first= |last= |authorlink= |coauthors= |title=Mystery DR Congo fever kills 100 |url=http://news.bbc.co.uk/2/hi/africa/6973013.stm |work= BBC News |publisher= |date=2007-08-31 |accessdate = 2008-02-25 ]On
November 30 ,2007 , theUganda Ministry of Health confirmed an outbreak of Ebola in theBundibugyo District . After confirmation of samples tested by the United States National Reference Laboratories and the Centers for Disease Control, the World Health Organization confirmed the presence of a new species of "Ebolavirus". [cite news |first= |last= |authorlink= |coauthors= |title=Uganda: Deadly Ebola Outbreak Confirmed - UN |url=http://allafrica.com/stories/200711301070.html |work=UN News Service |publisher= |date=2007-11-30 |accessdate = 2008-02-25 ] The epidemic came to an official end onFebruary 20 2008 . While it lasted, 149 cases of this new strain were reported, and 37 of those led to deaths.Weaponization
Because of Ebola lethality and lack of approved
vaccine or treatment, Ebola is classified as aBiosafety Level 4 agent, as well as a Category Abioterrorism agent [cite journal |author=Hoenen T, Groseth A, Falzarano D, Feldmann H |title=Ebola virus: unravelling pathogenesis to combat a deadly disease |journal=Trends Mol Med |volume=12 |issue=5 |pages=206–15 |year=2006 |pmid=16616875 |doi=10.1016/j.molmed.2006.03.006 |url=http://linkinghub.elsevier.com/retrieve/pii/S1471-4914(06)00064-5] and aselect agent by the CDC.As a terrorist weapon, Ebola has been considered by members of
Japan 'sAum Shinrikyo cult , whose leader,Shoko Asahara , led about 40 members to Zaire in 1992 under the guise of offering medical aid to Ebola victims in what was presumably an attempt to acquire a sample of the virus. [cite paper |last= |first= |author= |authorlink= |coauthors= |title=Chronology of Aum Shinrikyo's CBW Activities |version= |publisher=Monterey Institute for International Studies |date= |url=http://cns.miis.edu/pubs/reports/pdfs/aum_chrn.pdf |format= |id= |accessdate= ]Popular culture
Two
Tom Clancy novels—"Executive Orders " and "Rainbow Six "—describe scenarios in which Ebola is used as a biological weapon.The "Reston ebolavirus" is the subject of
Richard Preston 's non-fiction book "The Hot Zone ". It also led to the development of the movie "Outbreak" (1995).The movie "
Ebola Syndrome " is based on Ebola.Ebola is used by scientists in "
28 Days Later " to create the Rage Virus.ee also
*
Bolivian haemorrhagic fever *
Bushmeat *
Crimean-Congo haemorrhagic fever (CCHF)* Dr.
Jonah Kule , (-December 4 ,2007 )* Dr.
Matthew Lukwiya (1957-December 5 ,2000 ), AUganda n doctor at the forefront of the 2000 outbreak.* Dr.
Ngoy Mushola * Dr.
C.J. Peters *
Epidemiology *
Marburg virus , the first known disease caused by afilovirus *
VHFs References
Notes
Bibliography
* cite book
last=McCormick M.D.
first=Joseph B.
authorlink=Joseph B. McCormick
coauthors=Fisher-Hoch M.D., Susan
editor=
others=Horvitz, Leslie Alan
title=Level 4: Virus Hunters of the CDC
origdate=
origyear=1996
origmonth=June
url=
format=
accessdate=2008-08-02
accessyear=
accessmonth=
edition="Updated edition" 3rd
date=
year=1999
month=
publisher=Barnes & Noble
location=
language=
isbn=9780760712085
oclc=
doi=
id=
* cite book
last=Preston
first=Richard
authorlink=Richard Preston
title=The Hot Zone, A Terrifying True Story
origdate=
origyear=1994
origmonth=
url=
format=
accessdate=2008-08-02
edition=
series=
volume=
date=1995-07-20
publisher=Anchor Books (Random House), Sagebrush Education Resources, Tandem Library Books
location=
language=
isbn=0-385-47956-5
oclc=
doi=
id=
* cite web
url=http://www.stanford.edu/group/virus/filo/ebor.html
title=Ebola Reston Outbreak Standford Honors Thesis
accessdate=2008-08-02
author=
last=Waterman
first=Tara
authorlink=
coauthors=
date=
year=1999
month=
format=
work=
publisher=Stanford University
pages=
language=
doi=
archiveurl=
archivedate=
quote=External links
Overviews* [http://www.ncbi.nlm.nih.gov/ICTVdb/ICTVdB/01.025.0.02.htm Database entry on genus "Ebolavirus"] -
ICTVdB * [http://www.itg.be/ebola/ Ebola Virus Haemorrhagic Fever] - Proceedings of an International Colloquium on Ebola Virus Infection and Other Haemorrhagic Fevers held in Antwerp, Belgium, 6-8 December, 1977
* [http://www.cdc.gov/ncidod/dvrd/spb/mnpages/dispages/ebola/qa.htm Questions and Answers about Ebola Hemorrhagic Fever] - Center for Disease Control (CDC), retrieved 10 July 2006
* [http://www.who.int/mediacentre/factsheets/fs103/en/index.html WHO Factsheet] - retrieved 10 July 2006
*
* [http://www.vrc.nih.gov/scientificupdates_ebola.htm Vaccine Research Center (VRC)] - Information concerning Ebola vaccine research studies
* [http://www.healthocrates.com/ebola-hemorrhagic-fever www.healthocrates.com] - Article about Ebola hemorrhagic fever
Outbreaks
*
*
* [http://www.cdc.gov/ncidod/dvrd/spb/mnpages/dispages/ebotabl.htm History of Ebola Outbreaks] - Centers for Disease Control Special Pathogens Branch, retrieved
2006-07-10 .* [http://www.cdc.gov/ncidod/dvrd/spb/mnpages/vhfmanual/entire.pdf Infection Control for Viral Hemorrhagic Fevers in the African Health Care Setting] - Center for Disease Control and Prevention, Atlanta, December 1998.
* [http://www.ird.fr/filomeeting2008/ Filovirus Global Symposium] - Filomeeting 2008
Life Cycle
* [http://biomarker.cdc.go.kr:8080/pathogen/pathogen_view_en.jsp?pclass=2&id=44 Biomarker Database] - information on Ebola
Infectivity
* [http://www.usamriid.army.mil/press%20releases/warfield_press_release.pdf U.S. Army Medical Research Institute of Infectious Diseases: Gene-Specific Ebola Therapies Protect Nonhuman Primates from Lethal Disease]
*
*
*
*
*
* [http://www.brettrussell.com/personal/what_are_the_chances_.html What is the probability of a dangerous strain of Ebola mutating and becoming airborne?] ­ Brett Russel, retrieved
2006-07-10 .
Wikimedia Foundation. 2010.