- Anesthesia
-
Not to be confused with Paresthesia.For other uses, see Anesthesia (disambiguation).
Anesthesia, or anaesthesia (see spelling differences; from Greek αν-, an-, "without"; and αἴσθησις, aisthēsis, "sensation"), traditionally meant the condition of having sensation (including the feeling of pain) blocked or temporarily taken away. It is a pharmacologically induced and reversible state of amnesia, analgesia, loss of responsiveness, loss of skeletal muscle reflexes or decreased stress response, or all simultaneously. This allows patients to undergo surgery and other procedures without the distress and pain they would otherwise experience. An alternative definition is a "reversible lack of awareness," including a total lack of awareness (e.g. a general anesthetic) or a lack of awareness of a part of the body such as a spinal anesthetic. The pre-existing word anesthesia was suggested by Oliver Wendell Holmes, Sr. in 1846 as a word to use to describe this state.[1]
Types of anesthesia include local anesthesia, regional anesthesia, general anesthesia, and dissociative anesthesia. Local anesthesia inhibits sensory perception within a specific location on the body, such as a tooth or the urinary bladder. Regional anesthesia renders a larger area of the body insensate by blocking transmission of nerve impulses between a part of the body and the spinal cord. Two frequently used types of regional anesthesia are spinal anesthesia and epidural anesthesia. General anesthesia refers to inhibition of sensory, motor and sympathetic nerve transmission at the level of the brain, resulting in unconsciousness and lack of sensation.[2] Dissociative anesthesia uses agents that inhibit transmission of nerve impulses between higher centers of the brain (such as the cerebral cortex) and the lower centers, such as those found within the limbic system.
Contents
History
Main article: History of general anesthesiaPlant derivatives
Throughout Europe, Asia, and the Americas a variety of Solanum species containing potent tropane alkaloids were used, such as mandrake, henbane, Datura metel, and Datura inoxia. Ancient Greek and Roman medical texts by Hippocrates, Theophrastus, Aulus Cornelius Celsus, Pedanius Dioscorides, and Pliny the Elder discussed the use of opium and Solanum species. In 13th century Italy, Theodoric Borgognoni used similar mixtures along with opiates to induce unconsciousness, and treatment with the combined alkaloids proved a mainstay of anesthesia until the nineteenth century. In the Americas coca was also an important anesthetic used in trephining operations. Incan shamans chewed coca leaves and performed operations on the skull while spitting into the wounds they had inflicted to anesthetize the site.[citation needed] Alcohol was also used, its vasodilatory properties being unknown. Ancient herbal anesthetics have variously been called soporifics, anodynes, and narcotics, depending on whether the emphasis is on producing unconsciousness or relieving pain.
The use of herbal anesthesia had a crucial drawback compared to modern practice—as lamented by Fallopius, "When soporifics are weak, they are useless, and when strong, they kill." To overcome this, production was typically standardized as much as feasible, with production occurring from specific locations (such as opium from the fields of Thebes in ancient Egypt). Anesthetics were sometimes administered in the "spongia somnifera", a sponge into which a large quantity of drug was allowed to dry, from which a saturated solution could be trickled into the nose of the patient. At least in more recent centuries, trade was often highly standardized, with the drying and packing of opium in standard chests, for example. In the 19th century, varying aconitum alkaloids from a variety of species were standardized by testing with guinea pigs. Trumping this method was the discovery of morphine, a purified alkaloid that could be injected by hypodermic needle for a consistent dosage. The enthusiastic reception of morphine led to the foundation of the modern pharmaceutical industry.[citation needed]
The first effective local anesthetic was cocaine. Isolated in 1859, it was first used by Karl Koller, at the suggestion of Sigmund Freud, in eye surgery in 1884.[1] German surgeon August Bier (1861–1949) was the first to use cocaine for intrathecal anesthesia in 1898.[3] Romanian surgeon Nicolae Racoviceanu-Piteşti (1860–1942) was the first to use opioids for intrathecal analgesia; he presented his experience in Paris in 1901.[3] A number of newer local anesthetic agents, many of them derivatives of cocaine, were synthesized in the 20th century, including eucaine (1900), amylocaine (1904), procaine (1905), and lidocaine (1943).
Early inhalational anesthetics
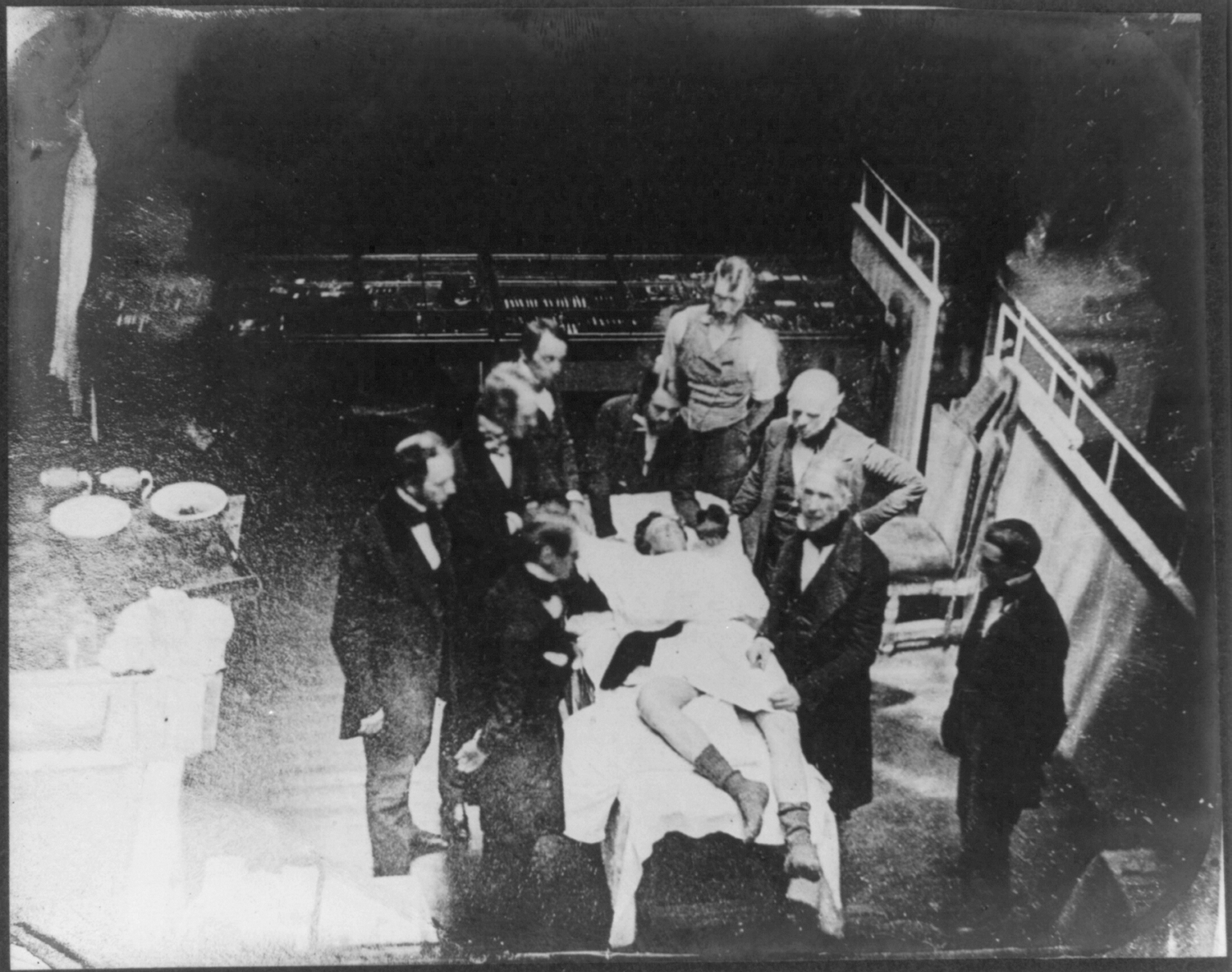
Further information: Inhalational anaesthetic Contemporary re-enactment of Morton's October 16, 1846, ether operation; daguerrotype by Southworth & Hawes
Contemporary re-enactment of Morton's October 16, 1846, ether operation; daguerrotype by Southworth & Hawes
The first physician to use diethyl ether as an anesthetic was Crawford Long, who administered it on 30 March 1842 during a surgical procedure to remove a tumor from a patient. He subsequently used it on multiple occasions afterward, but did not publish anything regarding the trials until 1849.[4]
William Thomas Green Morton, a Boston dentist, conducted the first public demonstration of the inhalational anesthetic. Morton, who was unaware of Long's previous work, was invited to the Massachusetts General Hospital to demonstrate his new technique for painless surgery. After Morton had induced anesthesia, surgeon John Collins Warren removed a tumor from the neck of Edward Gilbert Abbott. This occurred in the surgical amphitheater now called the Ether Dome. The previously skeptical Dr. Warren was impressed and stated "Gentlemen, this is no humbug." In a letter to Morton shortly thereafter, physician and writer Oliver Wendell Holmes, Sr. proposed naming the state produced "anesthesia", and the procedure an "anesthetic".[5]
Morton at first attempted to hide the actual nature of his anesthetic substance, referring to it as Letheon. He received a US patent for his substance, but news of the successful anesthetic spread quickly by late 1846. Respected surgeons in Europe including Liston, Dieffenbach, Pirogov, and Syme, quickly undertook numerous operations with ether. An American-born physician, Boott, encouraged London dentist James Robinson to perform a dental procedure on a Miss Lonsdale. This was the first case of an operator-anesthetist. On the same day, 19 December 1846, in Dumfries Royal Infirmary, Scotland, a Dr. Scott used ether for a surgical procedure.[citation needed] The first use of anesthesia in the Southern Hemisphere took place in Launceston, Tasmania, that same year. Drawbacks with ether such as excessive vomiting and its flammability led to its replacement in England with chloroform.
Discovered in 1831, the use of chloroform in anesthesia is linked to James Young Simpson, who, in a wide-ranging study of organic compounds, found chloroform's efficacy on 4 November 1847. Its use spread quickly and gained royal approval in 1853 when John Snow gave it to Queen Victoria during the birth of Prince Leopold. Unfortunately, chloroform is not as safe an agent as ether, especially when administered by an untrained practitioner (medical students, nurses, and occasionally members of the public were often pressed into giving anesthetics at this time). This led to many deaths from the use of chloroform that (with hindsight) might have been preventable. The first fatality directly attributed to chloroform anesthesia was recorded on 28 January 1848 after the death of Hannah Greener.[citation needed]
John Snow of London published articles from May 1848 onwards "On Narcotism by the Inhalation of Vapours" in the London Medical Gazette. Snow also involved himself in the production of equipment needed for the administration of inhalational anesthetics.
Anesthesia providers
Doctors specializing in perioperative care, development of an anesthetic plan, and the administration of anesthetics are known in the United States as anesthesiologists and in the United Kingdom and Canada as anaesthetists or anaesthesiologists. All anesthetics in the UK, Australia, New Zealand, Hong Kong and Japan are administered by doctors. Nurse anesthetists also administer anesthesia in 109 nations.[6] In the US, 35% of anesthetics are provided by physicians in solo practice, about 55% are provided by anesthesia care teams (ACTs) with anesthesiologists medically directing anesthesiologist assistants or certified registered nurse anesthetists (CRNAs), and about 10% are provided by CRNAs in solo practice.[7][8][9][10][11]
Physicians
Main article: Anesthesiologist Anesthesia students training with a patient simulator
Anesthesia students training with a patient simulatorIn the strict sense, the term anesthetist refers to any individual who administers anesthesia. In the US, however, the term is most commonly employed to refer to registered nurses who have completed specialized education and training in anesthesia to become certified registered nurse anesthetists (CRNAs). In the US and Canada, medical doctors who specialize in anesthesiology are called anesthesiologists. Such physicians in the United Kingdom (UK), Australia and New Zealand are called anaesthetists.
In the US, a physician specializing in anesthesiology typically completes four years of college, four years of medical school, and four years of postgraduate medical training or residency [12] According to the American Society of Anesthesiologists, anesthesiologists provide or participate in more than ninety percent of the forty million anesthetics delivered annually.[13] In the UK, this training lasts a minimum of seven years after the awarding of a medical degree and two years of basic residency, and takes place under the supervision of the Royal College of Anaesthetists.[citation needed] In Australia and New Zealand, it lasts five years after the awarding of a medical degree and two years of basic residency, under the supervision of the Australian and New Zealand College of Anaesthetists.[14] Other countries have similar systems, including Ireland (the Faculty of Anaesthetists of the Royal College of Surgeons in Ireland), Canada and South Africa (the College of Anaesthetists of South Africa).
In the US, satisfactory completion of the written and oral Board examinations allows an anesthesiologist to be called a "Diplomate" of the American Board of Anesthesiology (or of the American Osteopathic Board of Anesthesiology, for osteopathic physicians). This is often referred to colloquially as being "Board Certified". In the UK, Fellowship of the Royal College of Anaesthetists (FRCA) is conferred upon medical doctors following satisfactory completion of the written and oral parts of the Royal College's examination.
The role of the anesthesiologist is no longer limited to the operation itself. Many anesthesiologists function as perioperative physicians, ensuring optimal analgesia and maintenance of physiologic homeostasis throughout the preoperative, intraoperative, and postoperative periods. Anesthesiologists may elect to subspecialize in anesthesia for particular types of surgery (cardiothoracic, obstetrical, neurosurgical, pediatric), regional anesthesia, acute or chronic pain medicine, or Intensive Care Medicine.
Anesthesia providers are often trained using full scale human simulators. The field was an early adopter of this technology and has used it to train students and practitioners at all levels for the past several decades. Notable centers in the United States can be found at the Johns Hopkins Medicine Simulation Center,[15] Harvard's Center for Medical Simulation,[16] Stanford,[17] The Mount Sinai School of Medicine HELPS Center in New York,[18] and Duke University.[19]
Nurse anesthetists
Main article: Nurse anesthetistIn the United States, advanced practice nurses specializing in the provision of anesthesia care are known as Certified Registered Nurse anesthetists (CRNAs). According to the American Association of Nurse Anesthetists, the 39,000 CRNAs in the US administer approximately 30 million anesthetics each year, roughly two thirds of the US total.[20] 34% of nurse anesthetists practice in communities of less than 50,000. CRNAs start school with a bachelors degree and at least 1 year of acute care nursing experience,[21] and gain a masters degree in nurse anesthesia before passing the mandatory Certification Exam. Masters-level CRNA training programs range in length from 24 to 36 months.
CRNAs may work with podiatrists, dentists, anesthesiologists, surgeons, obstetricians and other professionals requiring their services. CRNAs administer anesthesia in all types of surgical cases, and are able to apply all the accepted anesthetic techniques—general, regional, local, or sedation. 34 states require physician supervision of a CRNA's practice, and hospitals can regulate what CRNAs can or can not do based on local laws.[22]
In the United States, the Centers for Medicare and Medicaid Services (CMS), a federal agency within the United States Department of Health and Human Services, determines the conditions for payment for all anesthesia services provided under the Medicare, Medicaid, and State Children's Health Insurance Program (SCHIP) programs. For the purposes of payment for anesthesiology services, CMS defines an anesthesia practitioner as a physician who performs the anesthesia service alone, a CRNA who is not medically directed, or a CRNA or AA who is medically directed.[23] Under the QZ Anesthesia Claims Modifier, CMS allows payment to a CRNA for anesthesiology services provided under these programs without medical direction by a physician.[23] Furthermore, under CMS regulations, anesthesia must be administered only by:
- a qualified doctor of medicine or osteopathic medicine, dentist, oral surgeon, or podiatrist;
- a CRNA who, unless exempted, is under the supervision of the operating practitioner or of an anesthesiologist;
- an anesthesiologist's assistant who is under the supervision of an anesthesiologist.[24]
The aforementioned exemption for CRNAs is the State exemption (also referred to as an "opt-out"). Under the State exemption, if the State in which the hospital is located submits a letter to CMS requesting exemption from physician supervision of CRNAs, and that letter has been signed by the Governor of that State, then hospitals within that State may be exempted from the requirement for physician supervision of CRNAs.[24] In 2001, CMS established this exemption for CRNAs from the physician supervision requirement by recognizing a Governor's written request to CMS attesting that it is in the best interests of the State's citizens to exercise this exemption.[25] As of September 2010, sixteen states (California, Iowa, Nebraska, Idaho, Minnesota, New Hampshire, New Mexico, Kansas, North Dakota, Washington, Alaska, Oregon, South Dakota, Wisconsin, Montana and Colorado) have chosen to opt-out of the CRNA physician supervision regulation.[25]
Anesthesiologist assistants
In the United States, anesthesiologist assistants (AAs) are graduate-level trained specialists who have undertaken specialized education and training to provide anesthesia care under the direction of an anesthesiologist. AAs typically hold a masters degree and practice under anesthesiologist supervision in 18 states and the District of Columbia through licensing, certification or physician delegation.[26]
In the UK, a similar group of assistants are currently being evaluated. They are referred to as "physician assistant (anaesthesia)" (PAA). Their background can be nursing, operating department practice, another of the allied medical professions, or even one of the natural sciences.[citation needed] Training is in the form of a postgraduate diploma and takes 27 months to complete.[citation needed]
Operating department practitioners
Main article: Operating Department PractitionersIn the United Kingdom, operating department practitioners provide assistance and support to the anesthetist or anesthesiologist. They can also assist the surgeon with surgical procedures and provide postoperative care to patients emerging from anesthesia. ODPs can be found in the operating department, accident and emergency department, intensive care unit, high dependency unit and in radiology, cardiology and endoscopy suites which require anesthesia support. They may also work with organ transplantation teams, as well as provide pre-hospital care to trauma victims. They are state-registered in the UK. The ODP is a mid-level practitioner of perioperative medicine. ODPs also function as lecturers and trainers in cardiopulmonary resuscitation, and work in management positions in operating departments.
Veterinary anesthetists/anesthesiologists
Main article: Veterinary anesthesiaMuch of the equipment and drugs utilized by veterinary anesthetists is similar or identical to that used in anesthesia for human patients. There are vast differences in the physiology of different animal species, which may influence the choice of anesthetic agents and delivery systems in organisms ranging in diversity from (for example) annelids to elephants. For many wild animals, anesthetic drugs must often be delivered from a distance by means of remote projector systems ("dart guns") before the animal can even be approached. Large domestic livestock can often be anesthetized for certain types of surgery in the standing position using only local anesthetics and sedative drugs. While most clinical veterinarians and veterinary technicians routinely function as anesthetists in the course of their professional duties, veterinary anesthesiologists in the U.S. are veterinarians who have completed a three year residency in anesthesia and have qualified for certification by the American College of Veterinary Anesthesiologists.
Other personnel
Further information: Anaesthetic technician, Biomedical Equipment Technician, and Surgical technologistAnesthesia technicians are specially trained biomedical technicians. They do not administer anesthesia, but rather they assist anesthesia providers similar to the way in which scrub technicians assist surgeons. Commonly these services are collectively called perioperative services, and thus the term perioperative service technician (PST) is used interchangeably with anesthesia technician. In the United States, an anesthesia technician can become a Certified Anesthesia Technician (Cer.A.T.), followed by becoming a Certified Anesthesia Technologist (Cer.A.T.T.) through American Society of Anesthesia Technologists & Technicians (ASATT).[27] In New Zealand, an anesthetic technician completes a course of study recognized by the New Zealand Anaesthetic Technicians Society.[28]
Anesthetic agents
Further information: Anesthetic, General anaesthetic, Inhalational anaesthetic, and Local anestheticAn anesthetic agent is a drug that brings about a state of anesthesia. A wide variety of drugs are used in modern anesthetic practice. Many are rarely used outside of anesthesia, although others are used commonly by all disciplines. Anesthetics are categorized in to two categories: general anesthetics cause a reversible loss of consciousness (general anesthesia), while local anesthetics cause reversible local anesthesia and a loss of nociception.
Anesthetic equipment
Main article: Instruments used in anesthesiologyIn modern anesthesia, a wide variety of medical equipment is desirable depending on the necessity for portable field use, surgical operations or intensive care support, and the type(s) of anesthetic(s) to be administered. Anesthesia practitioners must possess a comprehensive and intricate knowledge of the production and use of various medical gases, anesthetic agents and vapors, medical breathing circuits and the variety of anesthetic machines (including vaporizers, ventilators and pressure gauges) and their corresponding safety features, hazards and limitations of each piece of equipment, for the safe, clinical competence and practical application for day to day practice. The risk of transmission of infection by anesthetic equipment has been a problem since the beginnings of anesthesia. Although most equipment that comes into contact with patients is disposable, there is still a risk of contamination from the anesthetic machine itself[29] or because of bacterial passage through protective filters.[30]
Anesthetic monitoring
Patients under general anesthesia must undergo continuous physiological monitoring to ensure safety. In the US, the American Society of Anesthesiologists (ASA) have established minimum monitoring guidelines for patients receiving general anesthesia, regional anesthesia, or sedation. This includes electrocardiography (ECG), heart rate, blood pressure, inspired and expired gases, oxygen saturation of the blood (pulse oximetry), and temperature.[31] In the UK the Association of Anaesthetists (AAGBI) have set minimum monitoring guidelines for general and regional anesthesia. For minor surgery, this generally includes monitoring of heart rate, oxygen saturation, blood pressure, and inspired and expired concentrations for oxygen, carbon dioxide, and inhalational anesthetic agents. For more invasive surgery, monitoring may also include temperature, urine output, blood pressure, central venous pressure, pulmonary artery pressure and pulmonary artery occlusion pressure, cardiac output, cerebral activity, and neuromuscular function. In addition, the operating room environment must be monitored for ambient temperature and humidity, as well as for accumulation of exhaled inhalational anesthetic agents, which might be deleterious to the health of operating room personnel.
Effective July 1, 2011, the ASA implemented updated standards for patient monitoring.[32]
Anesthesia record
The anesthesia record is the medical and legal documentation of events while a patient is under anesthesia.[33] It reflects a detailed and continuous account of drugs, fluids, and blood products administered and procedures undertaken, and also includes the observation of cardiovascular responses, estimated blood loss, urine output and data from physiologic monitors (see "Anesthetic monitoring" section above) while a patient is under anesthesia.
Traditionally handwritten on paper, the anesthesia record is increasingly being replaced by an electronic record as part of an Anesthesia Information Management System (AIMS), especially since 2007.[34] An AIMS is any information system that is used as an automated electronic anesthesia record keeper (i.e., connection to patient physiologic monitors and/or the anesthetic machine) and which also may allow the collection and analysis of anesthesia-related perioperative patient data gathered from monitors and/or the anesthesia machine. These systems typically run on medical-grade hardware in the operating room. AIMS can be stand-alone systems or integrated modules of a hospital information system. AIMS have several benefits to the anesthesia departments as well to the hospital administration as documented in the scientific literature:
- Reducing anesthesia-related drug costs[35]
- Increased anesthesia billing and capture of anesthesia-related charges[36]
- Increased hospital reimbursement through improved hospital coding[37][38]
- Improvement of the data quality of the intraoperative anesthesia record[39][40]
- Support training and education of the anesthesia workforce[41]
- Support of clinical decision-making[42]
- Support of patient care and safety[43]
- Enhancement of clinical studies[44]
- Enhancement of clinical quality improvement programs[45]
- Support of clinical risk management[46]
- Monitoring for diversion of controlled substances[47]
See also
- Allergic reactions during anesthesia
- Anesthesia awareness
- ASA physical status classification system
- Cardiothoracic anesthesiology
- Geriatric anesthesia
- Intraoperative neurophysiological monitoring
- The Helsinki Declaration for Patient Safety in Anaesthesiology
- Patient safety
- Perioperative mortality
- Second gas effect
References
- ^ a b Morris Fishbein, ed (1976). "Anesthesia". The New Illustrated Medical and Health Encyclopedia. 1 (Home Library ed.). New York: H. S. Stuttman Co. pp. 87–9.
- ^ Career as an anaesthesiologist. Institute for career research. 2007. p. 1. ISBN 9781585111053. http://www.google.com/books?id=vQb5LnDI5CoC&dq=anesthesia+ancient&lr=&as_brr=3&source=gbs_navlinks_s. Retrieved 2010-11-25.
- ^ a b Brill S, Gurman GM and Fisher A (2003). "A history of neuraxial administration of local analgesics and opioids". European Journal of Anaesthesiology 20 (9): 682–9. doi:10.1017/S026502150300111X. ISSN 0265-0215. PMID 12974588.
- ^ Long C. W. (1849). "An account of the first use of Sulphuric Ether by Inhalation as an Anaesthetic in Surgical Operations". Southern Medical and Surgical Journal 5: 705–713.
- ^ Fenster, JM (2001). Ether Day: The Strange Tale of America's Greatest Medical Discovery and the Haunted Men Who Made It. New York: HarperCollins. ISBN 9780060195236.
- ^ "Nurse anesthesia worldwide: practice, education and regulation". International Federation of Nurse Anesthetists. http://ifna-int.org/ifna/e107_files/downloads/Practice.pdf. Retrieved 2010-11-25.
- ^ "Is Physician Anesthesia Cost-Effective?". Anesthesia and Analgesia. 2007. http://www.anesthesia-analgesia.org/cgi/content/full/98/3/750#R7-138848. Retrieved 2010-11-25.
- ^ Rosenbach, ML; Cromwell, J (2007). "When do anesthesiologists delegate?". Med Care 27 (5): 453–65. doi:10.1097/00005650-198905000-00002. PMID 2725080.
- ^ "Nurse anestheisa worldwide: practice, education and regulation". International Federation of Nurse Anesthetists. http://ifna-int.org/ifna/e107_files/downloads/Practice.pdf. Retrieved 2010-11-25.
- ^ "Surgical mortality and type of anesthesia provider". AANA. 2007. http://www.aana.com/news.aspx?ucNavMenu_TSMenuTargetID=171&ucNavMenu_TSMenuTargetType=4&ucNavMenu_TSMenuID=6&id=1606&terms=medical+direction+percent&searchtype=1&fragment=True. Retrieved 2010-11-25.
- ^ "Anesthesia Providers, Patient Outcomes, and Cost". Anesthesia and Analgesia. 2007. http://nursing.fiu.edu/anesthesiology/COURSES/Semester%203/NGR%206760%20ANE%20Prof%20Aspects/PROF%20Readings/Abenstein.pdf. Retrieved 2010-11-25.
- ^ ACGME Program Requirements for Graduate Medical Education in Anesthesiology, Effective: July 1, 2008
- ^ "ASA Fast Facts: Anesthesiologists Provide Or Participate In 90 Percent Of All Annual Anesthetics". ASA. http://www.asahq.org/PressRoom/homepage.html. Retrieved 2010-11-25.
- ^ "Australian and New Zealand College of Anaesthetists". College website. http://www.anzca.edu.au.
- ^ "Johns Hopkins Medicine Simulation Center". http://www.hopkinsmedicine.org/simulation_center/index.html. Retrieved 2010-11-25.
- ^ "The Center for Medical Simulation". Cambridge, Massachusetts. 2009. http://www.harvardmedsim.org/. Retrieved 2010-11-25.
- ^ "MedSim-Eagle Patient Simulator – Simulation Center". Stanford University School of Medicine. http://med.stanford.edu/VAsimulator/medsim.html. Retrieved 2010-11-25.
- ^ "Mount Sinai Simulation HELPS Center". http://msmc.affinitymembers.net/simulator/intro2.html. Retrieved 2010-11-25.
- ^ "Simcenter". http://simcenter.duke.edu/. Retrieved 2010-11-25.
- ^ About. AANA. Retrieved on 2010-09-29.
- ^ Becoming a CRNA. AANA. Retrieved on 2010-09-29.
- ^ Fact Sheet: Concerning State Opt Outs. AANA. Retrieved on 2010-09-29.
- ^ a b Centers for Medicare and Medicaid Services, Department of Health and Human Services (2010). "Chapter 12, Section 50: Payment for Anesthesiology Services". Medicare Claims Processing Manual. Washington, DC: U.S. Government Printing Office. pp. 116–23. http://www.cms.gov/manuals/downloads/clm104c12.pdf. Retrieved 2010-11-25.
- ^ a b Centers for Medicare and Medicaid Services, Department of Health and Human Services (2002). "IV: 42CFR482.52: Condition of participation: Anesthesia services". Code of Federal Regulations, Title 42. 3. Washington, DC: U.S. Government Printing Office. pp. 490–1. http://edocket.access.gpo.gov/cfr_2002/octqtr/42cfr482.52.htm. Retrieved 2010-11-25.
- ^ a b Centers for Medicare and Medicaid Services (2010). "Conditions for Coverage (CfCs) & Conditions of Participations (CoPs): Spotlight". Washington, DC: Centers for Medicare and Medicaid Services. http://www.cms.gov/CFCsAndCoPs/02_Spotlight.asp. Retrieved 2010-11-25.
- ^ "Five facts about AAs". American Academy of Anesthesiologist Assistants. Archived from the original on 2006-09-26. http://web.archive.org/web/20060926091707/http://www.anesthetist.org/content/view/14/38/. Retrieved 2010-11-25.
- ^ "ASATT Certification Information". American Society of Anesthesia Technologists & Technicians. http://www.asatt.org/cert.html. Retrieved 2010-11-25.
- ^ New Zealand Anaesthetic Technicians Society
- ^ Baillie, JK; P. Sultan, E. Graveling, C. Forrest, C. Lafong (2007). "Contamination of anaesthetic machines with pathogenic organisms". Anaesthesia 62 (12): 1257–61. doi:10.1111/j.1365-2044.2007.05261.x. PMID 17991263.
- ^ Scott, DHT; S Fraser, P Willson, G B Drummond, J K Baillie (2010). "Passage of pathogenic microorganisms through breathing system filters used in anaesthesia and intensive care". Anaesthesia 65 (7): 670–3. doi:10.1111/j.1365-2044.2010.06327.x. PMID 20374232.
- ^ STANDARDS FOR BASIC ANESTHETIC MONITORING. Committee of Origin: Standards and Practice Parameters (Approved by the ASA House of Delegates on October 21, 1986, and last amended on October 20, 2010 with an effective date of July 1, 2011)
- ^ http://www.beckershospitalreview.com/anesthesia/asas-standards-revision-focusing-on-ventilation-methods-goes-into-effect-july-1.html
- ^ Stoelting RK, Miller RD: Basics of Anesthesia, 3rd edition, 1994.
- ^ . doi:10.1213/ane.0b013e31818322d2.
- ^ Gillerman, RG; Browning, RA (2000). "Drug use inefficiency: a hidden source of wasted health care dollars". Anesthesia and Analgesia 91 (4): 921–4. doi:10.1097/00000539-200010000-00028. PMID 11004049.
- ^ Reich, DL; Kahn, RA; Wax, D; Palvia, T; Galati, M; Krol, M (2006). "Development of a module for point-of-care charge capture and submission using an anesthesia information management system". Anesthesiology 105 (1): 179–86; quiz 231–2. doi:10.1097/00000542-200607000-00028. PMID 16810010.
- ^ Martin, J; Ederle, D; Milewski, P (2002). "CompuRecord-A perioperative information management-system for anesthesia". Anasthesiologie, Intensivmedizin, Notfallmedizin, Schmerztherapie : AINS 37 (8): 488–91. doi:10.1055/s-2002-33172. PMID 12165922.
- ^ Meyer-Jark, T; Reissmann, H; Schuster, M; Raetzell, M; Rösler, L; Petersen, F; Liedtke, S; Steinfath, M et al. (2007). "Realisation of material costs in anaesthesia. Alternatives to the reimbursement via diagnosis-related groups". Der Anaesthesist 56 (4): 353–5. doi:10.1007/s00101-007-1136-6. PMID 17277957.
- ^ Cook, RI; McDonald, JS; Nunziata, E (1989). "Differences between handwritten and automatic blood pressure records". Anesthesiology 71 (3): 385–90. doi:10.1097/00000542-198909000-00013. PMID 2774266.
- ^ Devitt, JH; Rapanos, T; Kurrek, M; Cohen, MM; Shaw, M (1999). "The anesthetic record: accuracy and completeness". Canadian Journal of Anesthesia 46 (2): 122–8. doi:10.1007/BF03012545. PMID 10083991.
- ^ Edsall, DW (1991). "Computerization of anesthesia information management—users' perspective". Journal of Clinical Monitoring 7 (4): 351–8. doi:10.1007/BF01619360. PMID 1744682.
- ^ Merry AF, Webster CS, Mathew DJ (2001). "A new, safety-oriented, integrated drug administration and automated anesthesia record system". Anesthesia and Analgesia 93 (2): 385–90. doi:10.1097/00000539-200108000-00030. http://www.anesthesia-analgesia.org/content/93/2/385.full. Retrieved 2010-11-25.
- ^ O'Reilly, M; Talsma, A; Vanriper, S; Kheterpal, S; Burney, R (2006). "An anesthesia information system designed to provide physician-specific feedback improves timely administration of prophylactic antibiotics". Anesthesia and Analgesia 103 (4): 908–12. doi:10.1213/01.ane.0000237272.77090.a2. PMID 17000802.
- ^ Hollenberg, JP; Pirraglia, PA; Williams-Russo, P; Hartman, GS; Gold, JP; Yao, FS; Thomas, SJ (1997). "Computerized data collection in the operating room during coronary artery bypass surgery: a comparison to the hand-written anesthesia record". Journal of Cardiothoracic and Vascular Anesthesia 11 (5): 545–51. doi:10.1016/S1053-0770(97)90001-X. PMID 9263082.
- ^ Röhrig, R; Junger, A; Hartmann, B; Klasen, J; Quinzio, L; Jost, A; Benson, M; Hempelmann, G (2004). "The incidence and prediction of automatically detected intraoperative cardiovascular events in noncardiac surgery". Anesthesia and Analgesia 98 (3): 569–77. PMID 14980900.
- ^ Feldman, JM (2004). "Do anesthesia information systems increase malpractice exposure? Results of a survey". Anesthesia and Analgesia 99 (3): 840–3. doi:10.1213/01.ANE.0000130259.52838.3B. PMID 15333420.
- ^ Epstein, RH; Gratch, DM; Grunwald, Z (2007). "Development of a scheduled drug diversion surveillance system based on an analysis of atypical drug transactions". Anesthesia and Analgesia 105 (4): 1053–60, table of contents. doi:10.1213/01.ane.0000281797.00935.08. PMID 17898387.
Further reading
- Wolf, Jacqueline H. Deliver Me from Pain: Anesthesia and Birth in America (Johns Hopkins University Press, 2009) 277pp; covers 1840s to 21st century; ISBN 978-0-8018-9110-6
External links
Medical Specialities Specialties
and
subspecialtiesCardiac surgery · Cardiothoracic surgery · Colorectal surgery · General surgery · Neurosurgery · Ophthalmology · Oral and maxillofacial surgery · Orthopedic surgery · Hand surgery · Otolaryngology (ENT) · Pediatric surgery · Plastic surgery · Surgical oncology · Thoracic surgery · Transplant surgery · Trauma surgery · Urology · Vascular surgery
Allergy/Immunology · Andrology · Angiology (Vascular Medicine) · Cardiology · Endocrinology · Gastroenterology (Hepatology) · Geriatrics · Gynaecology · Hematology · Infectious disease · Nephrology · Oncology · Pulmonology · Rheumatology
DiagnosticHealthcare sciences (Clinical chemistry, Clinical immunology, Cytopathology, Medical microbiology, Transfusion medicine) · Radiology (Interventional radiology, Nuclear medicine) · Pathology (Anatomical, Clinical) · Clinical neurophysiology
Other specialtiesAddiction medicine · Adolescent medicine · Anesthesiology · Dermatology · Disaster medicine · Emergency medicine · Family medicine · General practice · Hospital medicine · Intensive-care medicine · Medical genetics · Neurology · Obstetrics · Occupational medicine · Pain management (Algiatry) · Palliative care · Pediatrics (Neonatology) · Physical medicine and rehabilitation (Physiatry) · Preventive medicine · Psychiatry · Radiation oncology · Reproductive medicine (Reproductive endocrinology and infertility, Reproductive surgery) · Sexual medicine · Sleep medicine · Sports medicine · Transplantation medicine · Tropical medicine (Travel medicine) · Urogynecology
Others Ancient anaesthesia Plants/animals Aconite • Castoreum • Cannabis • Coca • Deadly nightshade • Henbane • Lactucarium • Mandrake • Metel nut • Opium • Poison hemlock • Saussurea • Toloatzin • WillowPeople Abulcasis • Avenzoar • Avicenna • Celsus • Dioscorides • Galen • Hippocrates • Rhazes • Sabuncuoğlu • Sushrutha • Theophrastus • ZhangCompounds Aconitine • Δ9-THC • Atropine • Cocaine • Coniine • Hyoscyamine • Morphine • Salicylate • ScopolaminePain and nociception By region/system HEENTCardiovascular systemSore throat · PleurodyniaMusculoskeletalNeurologicCongenital insensitivity to pain · HSAN (Type I, II congenital sensory neuropathy, III familial dysautonomia, IV congenital insensitivity to pain with anhidrosis, V congenital insensitivity to pain with partial anhidrosis) · Neuralgia · Pain asymbolia · Pain disorder · Paroxysmal extreme pain disorder · Allodynia · Chronic pain · Hyperalgesia · Hypoalgesia · Hyperpathia · Phantom pain · Referred painUrogenitalGastrointestinalProctalgiaUpper · LowerTests Related concepts Anterolateral system · Pain management (Anesthesia, Cordotomy) · Pain scale · Pain threshold · Pain tolerance · Posteromarginal nucleus · Substance P · Suffering · OPQRST · Philosophy of pain · Cancer painCategories:

Wikimedia Foundation. 2010.