- Molluscum contagiosum
-
Molluscum contagiosum Classification and external resources 
Typical flesh-colored, dome-shaped and pearly lesionsICD-10 B08.1 ICD-9 078.0 DiseasesDB 8337 MedlinePlus 000826 eMedicine derm/270 MeSH D008976 Molluscum contagiousm virus 
EM of Molluscum contagiosum virus Virus classification Group: Group I (dsDNA) Family: Poxviridae Genus: Molluscipoxvirus Species: Molluscum contagiosum virus Molluscum contagiosum (MC) is a viral infection of the skin or occasionally of the mucous membranes. It is caused by a DNA poxvirus called the molluscum contagiosum virus (MCV). MCV has no animal reservoir, infecting only humans. There are four types of MCV, MCV-1 to -4; MCV-1 is the most prevalent and MCV-2 is seen usually in adults and often sexually transmitted. This common viral disease has a higher incidence in children, sexually active adults, and those who are immunodeficient,[1] and the infection is most common in children aged one to ten years old.[2] MC can affect any area of the skin but is most common on the trunk of the body, arms, and legs. It is spread through direct contact or shared items such as clothing or towels.
The virus commonly spreads through skin-to-skin contact. This includes sexual contact or touching or scratching the bumps and then touching the skin. Handling objects that have the virus on them (fomites), such as a towel, can also result in infection. The virus can spread from one part of the body to another or to other people. The virus can be spread among children at day care or at school. Molluscum contagiosum is contagious until the bumps are gone (which, if untreated, may last up to 6 months or longer).
The time from infection to the appearance of lesions can range up to 6 months, with an average incubation period between 2 and 7 weeks.[1]
Contents
Diagnosis
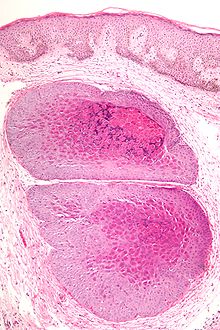
 High magnification micrograph of molluscum contagiosum, showing the characteristic molluscum bodies. H&E stain.
High magnification micrograph of molluscum contagiosum, showing the characteristic molluscum bodies. H&E stain.
Diagnosis is made on the clinical appearance; the virus cannot routinely be cultured. The diagnosis can be confirmed by excisional biopsy.
Histologically, molluscum contagiosum is characterized by molluscum bodies in the epidermis above the stratum basale, which consist of large cells with:
- abundant granular eosinophilic cytoplasm (accumulated virons), and
- a small peripheral nucleus.
Symptoms
Molluscum contagiosum lesions are flesh-colored, dome-shaped, and pearly in appearance. They are often 1–5 millimeters in diameter, with a dimpled center. They are generally not painful, but they may itch or become irritated. Picking or scratching the bumps may lead to further infection or scarring. In about 10% of the cases, eczema develops around the lesions. They may occasionally be complicated by secondary bacterial infections. In some cases the dimpled section may bleed once or twice.[citation needed] The viral infection is limited to a localized area on the topmost layer of the epidermis.[3] Once the virus containing head of the lesion has been destroyed, the infection is gone. The central waxy core contains the virus. In a process called autoinoculation, the virus may spread to neighboring skin areas. Children are particularly susceptible to autoinoculation, and may have widespread clusters of lesions.
Treatments
Individual molluscum lesions may go away on their own and are reported as lasting generally from 6 to 8 weeks,[4] to 2 or 3 months.[5] However via autoinoculation, the disease may propagate and so an outbreak generally lasts longer with mean durations variously reported as 8 months,[4] to about 18 months,[6][7] and with a range of durations from 6 months to 5 years.[5][7]
Treatment is often unnecessary[8] depending on the location and number of lesions, and no single approach has been convincingly shown to be effective. It should also be noted that treatments causing the skin on or near the lesions to rupture may spread the infection further, much the same as scratching does.[9] Nonetheless, treatment may be sought for the following reasons:
 Molluscum lesions on an arm.
Molluscum lesions on an arm.- Medical issues including:
- Bleeding
- Secondary infections
- Itching and discomfort
- Potential scarring
- Chronic keratoconjunctivitis
- Social reasons
- Cosmetic
- Embarrassment
- Fear of transmission to others
- Social exclusion
Many health professionals recommend treating bumps located in the genital area to prevent them from spreading.[7] The virus lives only in the skin and once the growths are gone, the virus is gone and cannot be spread to others. When treatment has resulted in elimination of all bumps, the infection has been effectively cured and will not reappear unless the patient is reinfected.[10] In practice, it may not be easy to see all of the molluscum contagiosum bumps. Even though they appear to be gone, there may be some that were overlooked. If this is the case, one may develop new bumps by autoinoculation, despite their apparent absence.
Cryotherapy
Cryotherapy involves killing infected cells by "freezing" them with a pressurized liquid spray, usually liquid nitrogen or nitrous oxide. The procedure can be mildly uncomfortable to painful depending on quantity and location of infected cells. The procedure can be performed by any medical professional.
Astringents
Astringent chemicals applied to the surface of molluscum lesions to destroy successive layers of the skin include trichloroacetic acid, podophyllin resin, potassium hydroxide, and cantharidin.[11]
Australian lemon myrtle
A 2004 study demonstrated over 90% reduction in the number of lesions in 9 out of 16 children treated once daily for 21 days with essential oil of Australian lemon myrtle (Backhousia citriodora) dissolved in olive oil.[12] However the oil may irritate normal skin at concentrations of 1%.[13][14]
Benzoyl peroxide
In a small randomized controlled trial twice daily application of 10% benzoyl peroxide cream for 4 weeks was found to be more effective than tretinoin 0.05% cream; after 6 weeks 92% of the benzoyl peroxide group were lesion-free, compared with 45% of the tretinoin group (p = 0.02)[15][16]
Cantharidin
Cantharidin is a chemical found naturally in many members of the beetle family Meloidae which causes dermal blistering. Cantharidin is not FDA approved but available through Canada or select US compounding pharmacy. Cantharidin does not cause pain upon application, and so it might be preferred by some when treating small children. It should probably not be used near the eyes or in uncooperative children, as the chemical is caustic if scratched and rubbed on the eyes. Cantharidin is usually applied with a wooden applicator like the sharp end of a wooden cotton bud. Some advocate leaving Cantharidin on unoccluded. Some advocate covering the molluscum bodies with tape for one to eight hours.[17] Extreme caution should be used when administering Cantharidin. Despite the fact that it is used as an aphrodisiac in some countries, it is highly toxic to humans if ingested.[18]
Tea tree oil
Another essential oil, tea tree oil is reported to at least reduce growth and spread of lesions when used in dilute form.[19] Tea tree oil may cause contact dermatitis to those with sensitive skin, although less often in dilute form.
Over-the-counter substances
For mild cases, over-the-counter wart medicines, such as salicylic acid may or may not[20] shorten infection duration. Daily topical application of tretinoin cream ("Retin-A 0.025%") may also trigger resolution.[21][22] These treatments require several months for the infection to clear, and are often associated with intense inflammation and possibly discomfort.
Imiquimod
Doctors occasionally prescribe Imiquimod, though the optimum schedule for its use has yet to be established.[23] Imiquimod is a form of immunotherapy. Immunotherapy triggers the immune system to fight the virus causing the skin growth. Imiquimod is applied 3 times per week, left on the skin for 6 to 10 hours, and washed off. A cure may take from 4 to 16 weeks. Small studies have indicated that it is successful about 80% of the time. Another dose regimen: apply imiquimod three times daily for 5 consecutive days each week.[24] Imiquimod has not been approved by the FDA as a treatment for molluscum contagiosum. This treatment regimen is reserved for 1% Imiquimod cream. If a higher concentration is used in a similar method, chemical burns or plausible nerve damage are possible.
Systemic treatments
Cimetidine (however, double blind placebo studies seem to refute this[25]), Griseofulvin (single case, anecdotal evidence) and Methisazone have seen some use.[5]
Surgical treatment
Surgical treatments include cryosurgery, in which liquid nitrogen is used to freeze and destroy lesions, as well as scraping them off with a curette. Application of liquid nitrogen may cause burning or stinging at the treated site, which may persist for a few minutes after the treatment. Scarring or loss of color can complicate both these treatments. With liquid nitrogen, a blister may form at the treatment site, but it will slough off in two to four weeks. Although its use is banned by the FDA in the United States in its pure, undiluted form, the topical blistering agent cantharidin can be effective.[26] Cryosurgery and curette scraping are not painless procedures. They may also leave scars and/or permanent white (depigmented) marks.
Laser
Pulsed dye laser therapy for molluscum contagiosum may be the treatment of choice for multiple lesions in a cooperative patient (Dermatologic Surgery, 1998). The use of pulsed dye laser for the treatment of MC has been documented with excellent results. The therapy was well tolerated, without scars or pigment anomalies. The lesions resolved without scarring at 2 weeks. Studies show 96%–99% of the lesions resolved with one treatment.[27][28] The pulsed dye laser is quick and efficient, but its expense makes it less cost effective than other options. Also, not all dermatology offices have this 585 nm laser.
Prognosis
Most cases of molluscum will clear up naturally within two years (usually within nine months). So long as the skin growths are present, there is a possibility of transmitting the infection to another person. When the growths are gone, the possibility for spreading the infection is ended.[10]
Unlike herpes viruses, which can remain inactive in the body for months or years before reappearing, molluscum contagiosum does not remain in the body when the growths are gone from the skin and will not reappear on their own.[10] However, there is no permanent immunity to the virus, and it is possible to become infected again upon exposure to an infected person.
Advantage of treatment is to hasten the resolution of the virus. This limits the size of the "pox" scar. If left untreated, molluscum growth can reach sizes as large as a pea or a marble. Spontaneous resolution of large lesions can occur, but will leave larger crater like growth. As many treatment options are available, prognosis for minimal scarring is best if treatment is initiated while lesions are small.
See also
- Acrochordons (also called skin tags — similar in appearance and grow in similar areas)
- Umbilicated lesions
References
- ^ a b Hanson D, Diven DG (March 2003). "Molluscum contagiosum". Dermatol. Online J. 9 (2): 2. PMID 12639455. http://dermatology.cdlib.org/92/reviews/molluscum/diven.html.
- ^ "Frequently Asked Questions: For Everyone. CDC Molluscum Contagiosum". United States Centers for Disease Control and Prevention. http://www.cdc.gov/ncidod/dvrd/molluscum/faq/everyone.htm#whogets. Retrieved 2008-06-29.
- ^ "Pamphlets: Molluscum Contagiosum". American Academy of Dermatology. 2006. http://www.aad.org/public/publications/pamphlets/viral_mollscum.html. Retrieved 2008-11-30.
- ^ a b Weller R, O'Callaghan CJ, MacSween RM, White MI (1999). "Scarring in molluscum contagiosum: comparison of physical expression and phenol ablation". BMJ 319 (7224): 1540. PMC 28297. PMID 10591712. http://www.bmj.com/cgi/content/full/319/7224/1540.
- ^ a b c Molluscum Contagiosum at eMedicine
- ^ MedlinePlus Encyclopedia Molluscum Contagiosum
- ^ a b c Tyring SK (2003). "Molluscum contagiosum: the importance of early diagnosis and treatment". Am. J. Obstet. Gynecol. 189 (3 Suppl): S12–6. doi:10.1067/S0002-9378(03)00793-2. PMID 14532898.
- ^ Prodigy knowledgebase (July 2003). "Molluscum Contagiosum". National Health Service. http://www.cks.nhs.uk/molluscum_contagiosum/management/scenario_molluscum_contagiosum#341804006. Retrieved 2010-04-20. - UK NHS guidelines on Molluscum Contagiosum
- ^ van der Wouden JC, Menke J, Gajadin S, et al. (2006). Van Der Wouden, Johannes C. ed. "Interventions for cutaneous molluscum contagiosum". Cochrane Database Syst Rev (2): CD004767. doi:10.1002/14651858.CD004767.pub2. PMID 16625612.
- ^ a b c "Frequently Asked Questions: For Everyone. CDC Molluscum Contagiosum". United States Centers for Disease Control and Prevention. http://www.cdc.gov/ncidod/dvrd/molluscum/faq/everyone.htm#howlongstay. Retrieved 2008-12-08.
- ^ "Molluscum Contagiosum - Treatment Overview". WebMD. January 12, 2007. http://www.webmd.com/skin-problems-and-treatments/tc/molluscum-contagiosum-treatment-overview. Retrieved 2007-10-21.
- ^ Burke BE, Baillie JE, Olson RD (2004). "Essential oil of Australian lemon myrtle (Backhousia citriodora) in the treatment of molluscum contagiosum in children". Biomed. Pharmacother. 58 (4): 245–7. doi:10.1016/j.biopha.2003.11.006. PMID 15183850.
- ^ Hayes AJ, Markovic B (2002). "Toxicity of Australian essential oil Backhousia citriodora (Lemon myrtle). Part 1. Antimicrobial activity and in vitro cytotoxicity". Food Chem. Toxicol. 40 (4): 535–43. doi:10.1016/S0278-6915(01)00103-X. PMID 11893412.
- ^ Hayes AJ, Markovic B (2003). "Toxicity of Australian essential oil Backhousia citriodora (lemon myrtle). Part 2. Absorption and histopathology following application to human skin". Food Chem. Toxicol. 41 (10): 1409–16. doi:10.1016/S0278-6915(03)00159-5. PMID 12909275.
- ^ http://cks.library.nhs.uk/molluscum_contagiosum/evidence/supporting_evidence/treatments_used_in_secondary_care_for_molluscum_contagiosum
- ^ Saryazdi S (2004). "The comparative efficacy of benzoyl peroxide 10% cream and tretinoin 0.05% cream in the treatment of molluscum contagiosum — Abstract: 10th World Congress on Pediatric Dermatology". Pediatric Dermatology 21 (3): 399.
- ^ http://www.emedsaver.com/index.php?pageID=0005&qryID=1&qry=Canthacur+Wart
- ^ Graziano MJ, Pessah IN, Matsuzawa M, Casida JE (June 1988). "Partial characterization of specific cantharidin binding sites in mouse tissues". Mol. Pharmacol. 33 (6): 706–12. PMID 3380085. http://molpharm.aspetjournals.org/cgi/pmidlookup?view=long&pmid=3380085.
- ^ aidsmap.com | Molluscum contagiosum
- ^ Schmitt, Jochen; Diepgen, Thomas L. (2008). "Molluscum contagiosum". In Berthold Rzany; Williams, Hywel; Bigby, Michael E.; Diepgen, Thomas L.; Herxheimer, Andrew; Luigi Naldi (PDF). Evidence-Based Dermatology. Evidence-based Medicine. London: BMJ Books. ISBN 1-4051-4518-8. http://www.blackwellpublishing.com/medicine/bmj/dermatology/pdfs/molluscum_contagiosum.pdf.
- ^ Papa C, Berger R (1976). "Venereal herpes-like molluscum contagiosum: treatment with tretinoin". Cutis 18 (4): 537–40. PMID 1037097.
- ^ Credo, BV; Dyment, PG (1996). "Molluscum Contagiosum". Adolesc Med 7 (1): 57–62. PMID 10359957.
- ^ Hanna D, Hatami A, Powell J, et al. (2006). "A prospective randomized trial comparing the efficacy and adverse effects of four recognized treatments of molluscum contagiosum in children". Pediatric dermatology 23 (6): 574–9. doi:10.1111/j.1525-1470.2006.00313.x. PMID 17156002.
- ^ Syed TA, Goswami J, Ahmadpour OA, Ahmad SA (May 1998). "Treatment of molluscum contagiosum in males with an analog of imiquimod 1% in cream: a placebo-controlled, double-blind study". J. Dermatol. 25 (5): 309–13. PMID 9640884.
- ^ Scheinfeld N (March 2003). "Cimetidine: a review of the recent developments and reports in cutaneous medicine". Dermatol. Online J. 9 (2): 4. PMID 12639457. http://dermatology.cdlib.org/92/reviews/cimetidine/scheinfeld.html.
- ^ Langley JM, Soder CM, Schlievert PM, Murray S (July 2003). "Case report: Molluscum contagiosum. Toxic shock syndrome following cantharidin treatment". Can Fam Physician 49: 887–9. PMC 2214253. PMID 12901485. http://www.cfp.ca/cgi/pmidlookup?view=long&pmid=12901485. "... although pure cantharidin and flexible collodion can be purchased as separate items and mixed by clinicians"
- ^ Hammes S, Greve B, Raulin C (2001). "Molluscum contagiosum: Treatment with pulsed dye laser" (in German). Der Hautarzt; Zeitschrift für Dermatologie, Venerologie, und verwandte Gebiete 52 (1): 38–42. PMID 11220237.
- ^ Hughes P (February 1998). "Treatment of molluscum contagiosum with the 585-nm pulsed dye laser". Dermatol Surg 24 (2): 229–30. doi:10.1016/S1076-0512(97)00178-7. PMID 9491117.
External links
- Molluscum Center for Disease Control
- Virus Pathogen Database and Analysis Resource (ViPR): Poxviridae
Sexually transmitted diseases and infections (STD/STI) (primarily A50–A64, 090–099) Bacterial Protozoal Parasitic Viral AIDS (HIV-1/HIV-2) · Cervical cancer, vulvar cancer & Genital warts (condyloma), Penile cancer, Anal cancer (Human papillomavirus (HPV)) · Hepatitis B (Hepatitis B virus) · Herpes simplex (HSV1/HSV2) · Molluscum contagiosum (MCV)General
inflammationInfectious skin disease: Viral cutaneous conditions, including viral exanthema (B00–B09, 050–059) HSV (Herpes simplex, Herpetic whitlow, Herpes gladiatorum, Herpetic keratoconjunctivitis, Herpetic sycosis, Neonatal herpes simplex, Herpes genitalis, Herpes labialis, Eczema herpeticum, Herpetiform esophagitis) · Herpes B virus (B virus infection)VZV (Chickenpox, Herpes zoster, Herpes zoster oticus, Ophthalmic zoster, Disseminated herpes zoster, Zoster-associated pain, Inflammatory skin lesions following zoster infection, Modified varicella-like syndrome)Human herpesvirus 6/Roseolovirus (Exanthema subitum, Roseola vaccinia)SealpoxOtherPapillomaviridaeHPV (Wart/Plantar wart, Heck's disease, Genital wart (giant), Laryngeal papillomatosis, Butcher's wart, Bowenoid papulosis, Epidermodysplasia verruciformis, Verruca plana, Pigmented wart, Verrucae palmares et plantares )
BPV (Equine sarcoid)Parvovirus B19 (Erythema infectiosum, Reticulocytopenia, Papular purpuric gloves and socks syndrome)CAV (Hand, foot and mouth disease, Herpangina) · FMDV (Foot-and-mouth disease) · Boston exanthem diseaseUngrouped unknown/multiple: Asymmetric periflexural exanthem of childhood · Post-vaccination follicular eruption · Lipschütz ulcer · Eruptive pseudoangiomatosis · Viral-associated trichodysplasia · Gianotti–Crosti syndromeCategories:- Poxviruses
- Sexually transmitted diseases and infections
- Virus-related cutaneous conditions





Wikimedia Foundation. 2010.